Gallbladder Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Gallbladder cancer is one of the most challenging gastrointestinal cancers — not because treatment options do not exist, but because it is almost always found either very late or unexpectedly. What happens in the first weeks after diagnosis shapes the outcome more than almost anything else. At CION Cancer Clinics, our hepatobiliary surgical and medical oncology team delivers the full spectrum of gallbladder cancer care across 7 Hyderabad locations, backed by 5-Star NABH accreditation and NCCN protocol-driven treatment planning.
4.8 · 800+ Google reviews · 15,000+ patients treated
Medically reviewed by Dr. Owais Mohammed, MBBS, MD · Authored by Dr. Paila Gowri Naidu, MCh Surgical Oncology · Last reviewed May 2026
17+
Cancer Specialists on Panel
96.9%
Breast Cancer Survival Rate*
15,000+
Patients Treated
4.8★
Google Rating (800+ reviews)
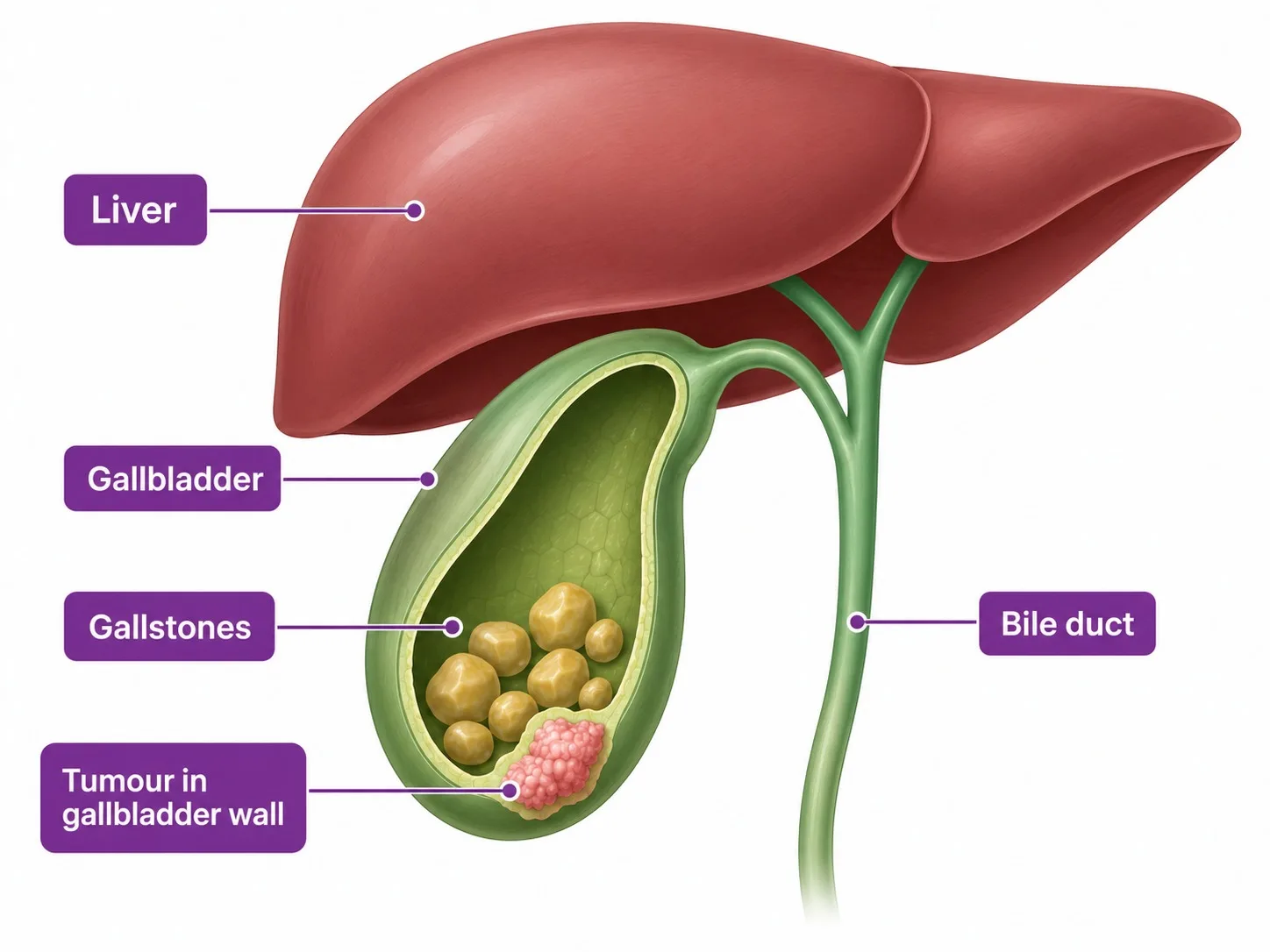
A Disease That Demands Specialist Care
Gallbladder Cancer in India
The gallbladder sits under the liver — long-standing gallstones are the main risk factor for gallbladder cancer.
India has one of the highest rates of gallbladder cancer in the world. The Indo-Gangetic belt — running through northern India — has an incidence as high as 21 cases per 100,000 people, among the highest globally. Across Telangana and Andhra Pradesh, incidence is lower but clinically meaningful, driven by the high prevalence of gallstone disease in the population.
Gallbladder cancer is aggressive and fast-growing — a challenge examined in this Mayo Clinic discussion of hidden gallbladder and bile duct cancers. The reason outcomes are often poor is not that effective treatment does not exist — it is that most patients present when the cancer has already grown beyond the gallbladder. Only approximately 10% of patients have disease that is surgically removable at the time of diagnosis. For those patients, surgery combined with chemotherapy offers a genuine chance of cure. For the majority, systemic chemotherapy aims to slow the cancer's growth and maintain quality of life.
The most important determinant of outcome is access to a specialist oncology team that knows this cancer, performs the correct extent of surgery when indicated, and starts chemotherapy promptly after resection.
Did You Know? Stone size matters as much as having stones at all.
Gallstones are the single biggest risk factor for gallbladder cancer — and stone size matters. People with gallstones larger than 3cm have a significantly higher risk than those with smaller stones. If you have been told you have large gallstones but have not had surgery, speak to an oncologist about your risk.
Risk Factors
What Causes Gallbladder Cancer and Who Is at Risk?
GallstonesThe most important risk factor; particularly single stones above 3cm. Chronic gallstone-related inflammation damages the gallbladder lining over years.
Female genderGallbladder cancer is 2–3 times more common in women than men — mirrors the higher prevalence of gallstone disease in women.
ObesityIncreases gallstone formation risk and is independently associated with gallbladder cancer.
Chronic cholecystitisLong-standing chronic gallbladder inflammation, with or without gallstones, raises cancer risk.
Porcelain gallbladderCalcium deposits in the gallbladder wall from chronic inflammation — surgical removal is generally recommended.
Gallbladder polyps above 1cmPolyps of this size carry a meaningful risk of malignancy and are generally recommended for surgical removal.
Abnormal pancreaticobiliary junction (APBJ)A congenital abnormality causing reflux of pancreatic juice into the bile duct — strongly associated with gallbladder cancer.
Family historyFamily history of gallbladder or biliary cancer increases risk.
Symptoms
Symptoms of Gallbladder Cancer
Gallbladder cancer is frequently called a 'silent' cancer — it produces no specific symptoms in its early stages. Most early-stage cancers are found incidentally, either during ultrasound for another condition or unexpectedly in the pathology specimen after routine gallstone surgery. When symptoms do occur, they often indicate more advanced disease:
Pain or discomfort in the upper right abdomen — can be persistent or intermittent; often initially attributed to gallstones
Jaundice — yellowing of the skin and eyes, dark urine, and pale stools; indicates the cancer has grown to involve the bile duct, blocking bile flow
Nausea, vomiting, and significant loss of appetite
Unexplained weight loss
Abdominal bloating or a lump felt in the upper right abdomen
Fever without infection — a sign of biliary obstruction or tumour-related inflammation
Jaundice from gallbladder cancer is a sign of locally advanced disease and requires urgent specialist evaluation. Do not delay — early-onset jaundice in patients with known gallstone disease should always prompt CT and oncology review.
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.
A complete diagnostic workup combines imaging, blood markers, and (where needed) tissue sampling — followed by tumour board review to plan the right treatment sequence.
01
Imaging
Ultrasound — first-line investigation; identifies gallbladder wall thickening, polyps, masses, and bile duct involvement
CT Scan (triphasic, with contrast) — the primary staging investigation; assesses gallbladder wall invasion, liver involvement, portal lymph nodes, bile duct involvement, and distant metastases
MRI / MRCP — for biliary anatomy assessment, bile duct involvement, and vascular relations; essential for surgical planning
PET-CT — for detecting distant metastases and assessing treatment response in recurrent disease
02
Tumour Markers
CA19-9 — elevated in most gallbladder cancers; used for diagnosis support, monitoring treatment response, and surveillance after surgery
CEA (carcinoembryonic antigen) — complementary marker; used alongside CA19-9
03
Biopsy & Molecular Testing
For confirmed gallbladder masses on imaging with raised CA19-9, biopsy is sometimes avoided before surgery to prevent seeding. When required — for unresectable disease before starting chemotherapy — CT-guided or EUS-guided biopsy is performed. Molecular testing of biopsy tissue (FGFR2 fusions, IDH1 mutations, HER2 status) is arranged for advanced disease to assess targeted therapy eligibility.
Staging
Gallbladder Cancer Staging and Survival Rates
Gallbladder cancer is staged using the AJCC TNM system. The T stage — how deeply the cancer has grown through the gallbladder wall — is the most important predictor of outcome and determines whether curative surgery is possible.
Extended radical resection where possible + adjuvant capecitabine
T4 / Stage IV
Major vessel invasion or distant spread
Portal vein, hepatic artery, or metastases
5–15%
Systemic chemotherapy (gemcitabine + cisplatin); palliative care
Note: 5-year survival estimates are for gallbladder adenocarcinoma treated at specialist centres. Outcomes are highly dependent on completeness of surgical resection and prompt adjuvant chemotherapy.
Incidental Gallbladder Cancer
When Gallstone Surgery Reveals More
One of the most common and most anxiety-inducing situations in gallbladder cancer — and one that no hospital treatment page in Hyderabad addresses — is incidental gallbladder cancer. This happens when a patient undergoes routine laparoscopic surgery for gallstones, and the removed gallbladder is sent for routine pathological examination, which reveals cancer that was not suspected before the operation.
This is not a rare situation. A small but significant proportion of gallbladders removed for routine gallstone disease are found to contain early cancer on pathological examination. What happens next depends entirely on the T stage:
Tis (carcinoma in situ) and T1a — simple laparoscopic cholecystectomy has already been curative; no further surgery is required. Regular surveillance with CA19-9 and imaging is arranged.
T1b — the cancer has grown into the muscle layer; simple cholecystectomy is not sufficient. Revision surgery — radical cholecystectomy with liver wedge resection, lymphadenectomy, and excision of the laparoscopic port sites — is required. Port site excision is important because laparoscopic instruments can seed cancer cells at the entry points during the initial operation.
T2 and T3 — revision surgery is required and more extensive; formal liver segment IVb + V resection alongside portal lymphadenectomy is the standard.
If you or a family member has received a pathology report after gallstone surgery that mentions cancer in the specimen — even if the surgeon said the operation was routine — this requires urgent review by a surgical oncologist specialising in hepatobiliary cancer. The window for curative revision surgery is time-sensitive.
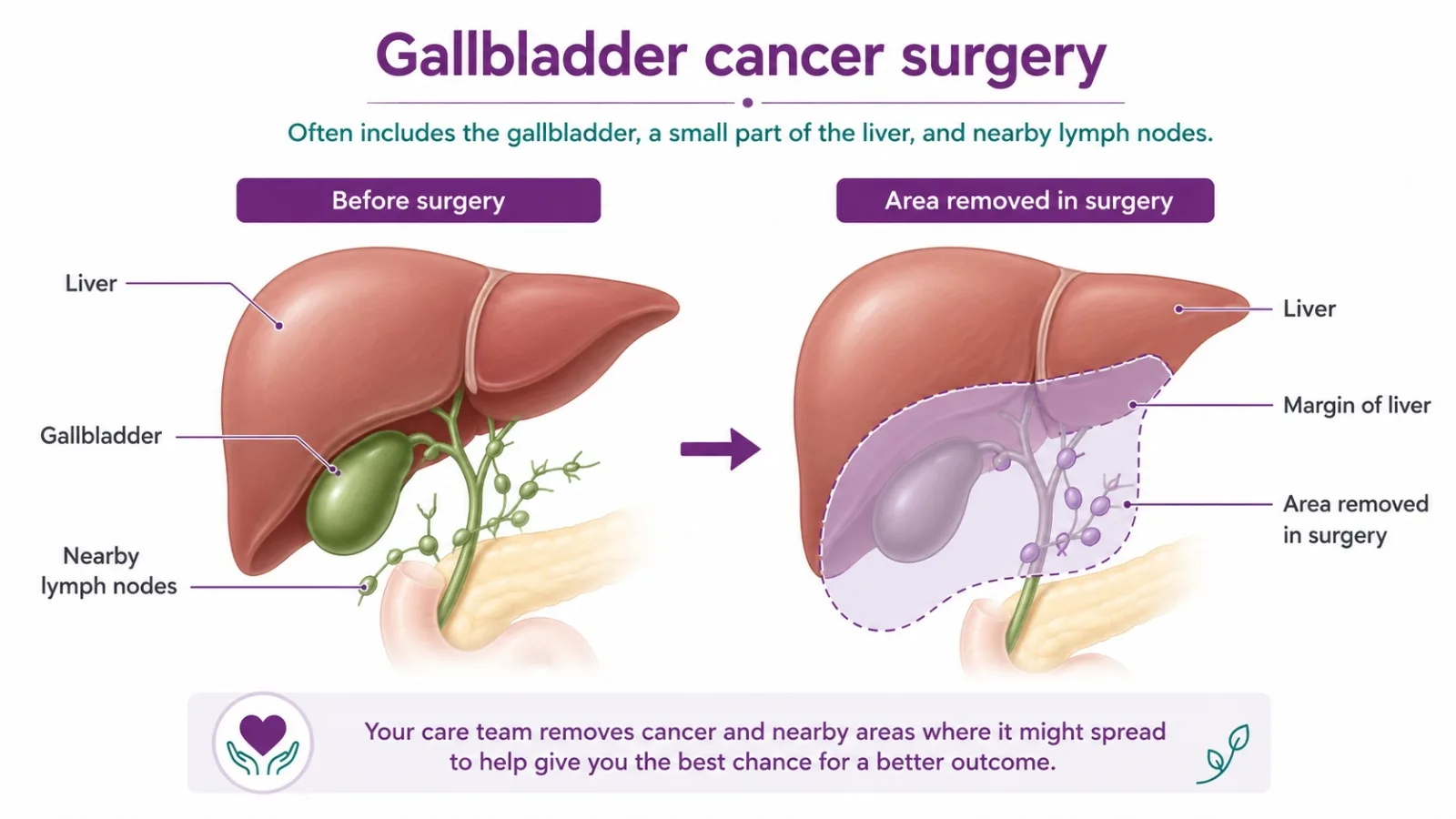
Radical vs Simple Cholecystectomy
Why Simple Cholecystectomy Is Not Enough
An extended cholecystectomy removes the gallbladder along with a margin of liver and nearby lymph nodes — more than a routine gallbladder removal.
This is the most important surgical distinction for gallbladder cancer — and the one most patients do not know to ask about. There is a critical difference between a simple cholecystectomy (removing just the gallbladder) and a radical cholecystectomy (the correct operation for gallbladder cancer from T1b onwards).
The gallbladder sits directly against the liver. Cancer cells that have grown through the gallbladder wall into the surrounding tissue will not be removed by simple cholecystectomy — they will be left behind, and the cancer will recur. The correct surgery removes:
The gallbladder
A 2cm wedge of liver tissue adjacent to the gallbladder bed (or formal liver segment IVb + V resection for deeper invasion)
All regional (portal) lymph nodes
The common bile duct where involved
The laparoscopic port sites — for incidental GBC discovered after laparoscopic surgery
This is a complex hepatobiliary procedure that requires a surgical oncologist with specific experience in liver and biliary surgery. CION's surgical oncology team, led by Dr. Paila Gowri Naidu (MCh Surgical Oncology, BHU Varanasi — one of India's leading hepatopancreaticobiliary surgery training institutions), performs radical cholecystectomy and revision surgery for incidental GBC as part of its hepatobiliary oncology pathway.
Systemic Therapy
Chemotherapy for Gallbladder Cancer — Before and After Surgery
Three distinct chemotherapy roles in gallbladder cancer treatment — each backed by landmark clinical trials and NCCN/ESMO recommendations.
Adjuvant Capecitabine (BILCAP)
After surgical resection — even when all visible cancer has been removed — microscopic cancer cells may remain. Oral capecitabine for 6 months significantly reduces recurrence risk. The BILCAP trial showed median overall survival improved from 36.4 months (observation) to 51.1 months with adjuvant capecitabine. NCCN and ESMO both recommend it for all patients from T1b onwards with complete resection.
Gemcitabine + Cisplatin (ABC-02)
For patients with locally advanced, unresectable, or metastatic gallbladder cancer — the majority of patients at diagnosis — systemic chemotherapy is the primary treatment. The combination of gemcitabine and cisplatin (the ABC-02 trial) is the standard first-line regimen, demonstrating significantly improved survival compared to gemcitabine alone. Delivered in a day-care setting with regular blood count and kidney function monitoring.
Second-Line & Targeted Therapy
For patients who progress on gemcitabine + cisplatin, second-line options include FOLFOX (oxaliplatin + 5-fluorouracil). Molecular testing of biopsy tissue — for FGFR2 fusions, IDH1 mutations, HER2 amplification, and MSI-H/dMMR status — identifies patients eligible for newer targeted therapies. CION arranges molecular profiling for all advanced gallbladder cancer patients at progression.
Did You Know? T1b and above means revision surgery — within weeks.
If gallbladder cancer is found in your pathology report after routine cholecystectomy for gallstones, the next step depends entirely on how deeply the cancer has grown. For T1b and above, revision surgery is necessary — and needs to be performed at a specialist hepatobiliary oncology centre within weeks of diagnosis. Simple removal of the gallbladder alone is not sufficient treatment for these stages.
Supportive Care
Supportive and Palliative Care for Advanced Disease
For patients with unresectable or metastatic gallbladder cancer, maintaining quality of life is as important as slowing disease progression. CION's integrated palliative care approach includes:
Biliary drainageEndoscopic (ERCP) or percutaneous biliary stenting for patients with obstructive jaundice — relieves jaundice, itching, and liver strain, and improves tolerance of chemotherapy.
Pain managementSpecialist pain control for right upper quadrant pain from tumour invasion.
Nutritional supportDietitian-led guidance to maintain weight and strength during chemotherapy.
Psychological supportOncology counselling for patients and families managing a difficult diagnosis.
Why Choose CION
Why Patients Choose CION for Gallbladder Cancer Treatment in Hyderabad
1,000+ gall bladder cancer cases treated every year across the CION network
Multidisciplinary tumour board review for every patient
Full integrative support — nutrition counselling and psychological support
Dedicated Second Opinion service
EMI facility — flexible payment options for all patients
4.8 / 5 rating across 800+ patient reviews
India's fastest-growing cancer care network — 35+ centres across Telangana and Andhra Pradesh
Treatment Cost
Gallbladder Cancer Treatment Cost in Hyderabad
Treatment costs vary depending on stage, extent of surgery required, and systemic therapy needed. The following ranges reflect current Hyderabad market data.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
Frequently Asked Questions — Gallbladder Cancer Treatment in Hyderabad
What are the symptoms of gallbladder cancer?
Gallbladder cancer often causes no symptoms in its early stages — which is why it is so often found incidentally after routine surgery for gallstones. When symptoms do appear, the most common are: persistent pain or discomfort in the upper right abdomen; jaundice (yellowing of the skin and eyes, dark urine, pale stools) — which indicates the cancer has grown to block the bile duct; nausea, vomiting, and loss of appetite; unexplained weight loss; abdominal bloating; and fever without infection. Jaundice from gallbladder cancer is a sign of advanced disease and requires same-week specialist review and imaging.
Is gallbladder cancer curable?
Yes — gallbladder cancer is curable, but only when detected at a stage where surgery can remove it completely. Very early disease (Tis and T1a) is cured by simple cholecystectomy alone, with 5-year survival rates of 85–100%. T1b and T2 disease treated with radical cholecystectomy (liver wedge + lymphadenectomy) followed by adjuvant capecitabine has 5-year survival of 50–80%. The challenge is that most gallbladder cancers are not detected at these early stages. This is why incidental discovery after gallstone surgery — while alarming — actually represents a genuine opportunity for cure when followed by prompt specialist management.
What causes gallbladder cancer?
The most important risk factor is gallstone disease — particularly large stones above 3cm. Gallstones cause chronic inflammation of the gallbladder lining, which over years increases cancer risk. Female gender (women have gallbladder cancer 2–3 times more often than men), obesity, chronic cholecystitis, porcelain gallbladder, gallbladder polyps above 1cm, and an abnormal pancreaticobiliary junction (a congenital condition causing reflux of pancreatic juice into the bile duct) are other established risk factors. India's high prevalence of gallstone disease explains its disproportionately high rate of gallbladder cancer compared to most of the world.
What is incidental gallbladder cancer?
Incidental gallbladder cancer is cancer discovered unexpectedly in the pathology report after routine laparoscopic cholecystectomy for gallstones. The gallbladder is sent for standard pathological examination after every cholecystectomy — and in a small proportion of cases, cancer is found that was not suspected before the operation. What happens next depends on how deeply the cancer has grown through the gallbladder wall (the T stage). T1a cancers are cured by the initial operation alone. T1b and above require a second, more extensive operation — revision surgery — to remove liver tissue, lymph nodes, and the laparoscopic port sites. If you have received a pathology report after gallstone surgery that mentions cancer, this requires urgent oncology review within 2–4 weeks.
What is radical cholecystectomy?
Radical cholecystectomy is the correct surgical operation for gallbladder cancer from T1b onwards. It involves removing: the gallbladder; a wedge of liver tissue adjacent to the gallbladder (or formal liver segment IVb + V resection for deeper tumours); all regional (portal) lymph nodes between the liver and pancreas; and sometimes part of the bile duct if it is involved. For incidental gallbladder cancer found after laparoscopic surgery, the laparoscopic port sites are also excised. Simple cholecystectomy — removing just the gallbladder — is not sufficient treatment for T1b and above, because cancer cells in the gallbladder wall or surrounding tissue will be left behind and the cancer will recur.
What is the survival rate for gallbladder cancer?
Survival rates depend critically on stage at diagnosis. Tis/T1a: 5-year survival 85–100% with simple cholecystectomy. T1b: 70–80% with radical cholecystectomy. T2 (Stage II): 50–70% with radical surgery and adjuvant capecitabine. T3 (Stage III): 20–40% with extended radical resection. Stage IV (distant spread): 5–15%. The poor overall survival statistics often quoted for gallbladder cancer reflect the fact that most patients are diagnosed at Stage III or Stage IV, when curative surgery is no longer possible. For patients diagnosed at early stages — including incidental discovery after gallstone surgery — outcomes are considerably better.
What is the treatment for advanced gallbladder cancer?
For advanced (unresectable or metastatic) gallbladder cancer, systemic chemotherapy with gemcitabine and cisplatin is the standard first-line treatment, based on the ABC-02 trial demonstrating improved overall survival compared to gemcitabine alone. Treatment typically continues for 6 months and is monitored with regular CT scans and tumour markers. For patients with jaundice from bile duct obstruction, biliary stenting (ERCP) is placed before chemotherapy to restore bile flow. Molecular testing of the tumour (FGFR2, IDH1, HER2, MSI-H) is arranged to identify patients eligible for targeted therapies at progression. Alongside chemotherapy, comprehensive palliative care manages pain, nutrition, and quality of life.
Can gallbladder cancer spread to the liver?
Yes — the liver is the most common site of gallbladder cancer spread, because the gallbladder sits directly against the liver bed. The cancer can grow through the gallbladder wall into adjacent liver tissue (T3 local invasion) or spread through the portal blood supply to form liver metastases (Stage IV). This is why the correct surgery for gallbladder cancer includes removal of a wedge of liver tissue alongside the gallbladder — not just the gallbladder itself. When cancer has spread widely through the liver, surgery is no longer curative and systemic chemotherapy becomes the primary treatment.
What is the cost of gallbladder cancer treatment in Hyderabad?
Costs in Hyderabad vary by stage and treatment. Radical cholecystectomy with liver wedge and lymphadenectomy costs approximately ₹2,50,000 to ₹6,00,000. Extended resection for T3 disease (liver segment IVb+V) costs ₹4,00,000 to ₹9,00,000. Revision surgery for incidental GBC costs ₹3,00,000 to ₹7,00,000. Adjuvant capecitabine (6-month oral course) costs ₹30,000 to ₹90,000 in total. Gemcitabine + cisplatin (IV chemotherapy for advanced disease) costs ₹30,000 to ₹80,000 per cycle. CION provides a personalised cost estimate after your initial oncology consultation. EMI payment options are available for all patients.
Can I get a second opinion for gallbladder cancer?
Absolutely — and for gallbladder cancer, a second opinion is particularly important in two situations. First, if you have received an incidental GBC diagnosis after gallstone surgery and been told no further treatment is needed — for T1b and above, this is almost certainly incorrect; revision surgery is required. Second, if advanced disease has been declared inoperable — the line between resectable and unresectable gallbladder cancer can be narrow and is best assessed by a surgical oncologist experienced specifically in hepatobiliary surgery. CION offers a dedicated Second Opinion service where our tumour board reviews your imaging, pathology, and existing recommendation before advising on the appropriate pathway forward.
Need a Second Opinion?
Free consultation with a specialist. No commitment.