Do you have to drink alcohol to get liver cancer?
No — this is a common myth. Alcohol is one cause, but in India the biggest causes are chronic hepatitis B and hepatitis C (often silent, sometimes caught at birth) and increasingly fatty liver (linked to obesity and diabetes). You can develop liver cancer without ever drinking, which is why getting tested for hepatitis B and C matters.
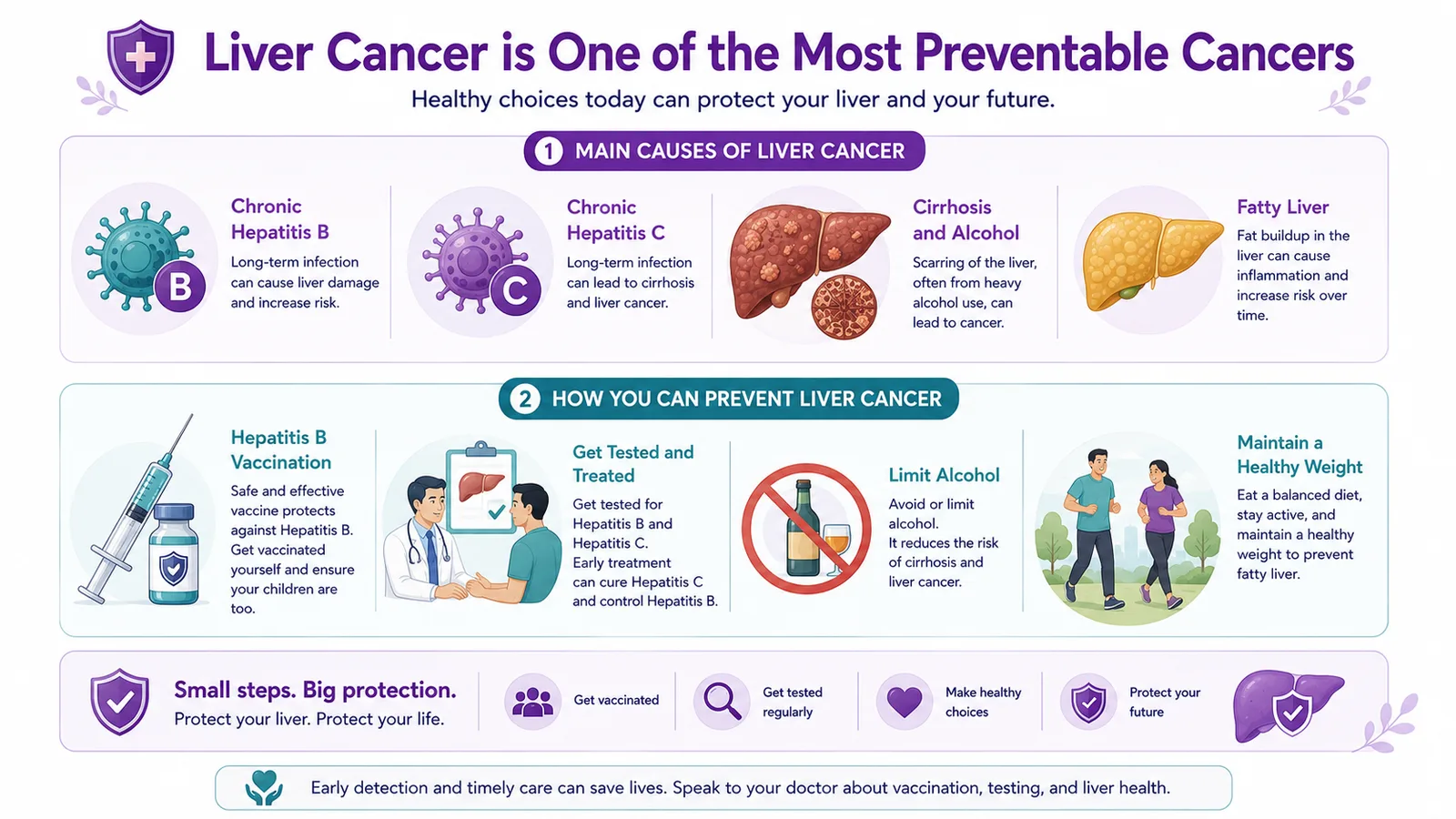
Can liver cancer be prevented?
To a large extent, yes. It is one of the most preventable cancers: the hepatitis B vaccine is safe and effective, hepatitis B and C can be tested for and treated (hepatitis C can be cured), and limiting alcohol and managing weight and fatty liver prevent much of the rest. And in people already at risk, 6-monthly surveillance catches it early.
I have hepatitis B or cirrhosis — will I get liver cancer?
Not necessarily — most people with hepatitis or cirrhosis never develop liver cancer, especially if the hepatitis is treated. But the risk is higher, so regular surveillance (a 6-monthly liver ultrasound and an AFP blood test) is strongly advised — it catches any cancer early, when it is most curable. Treating the hepatitis also lowers the risk.
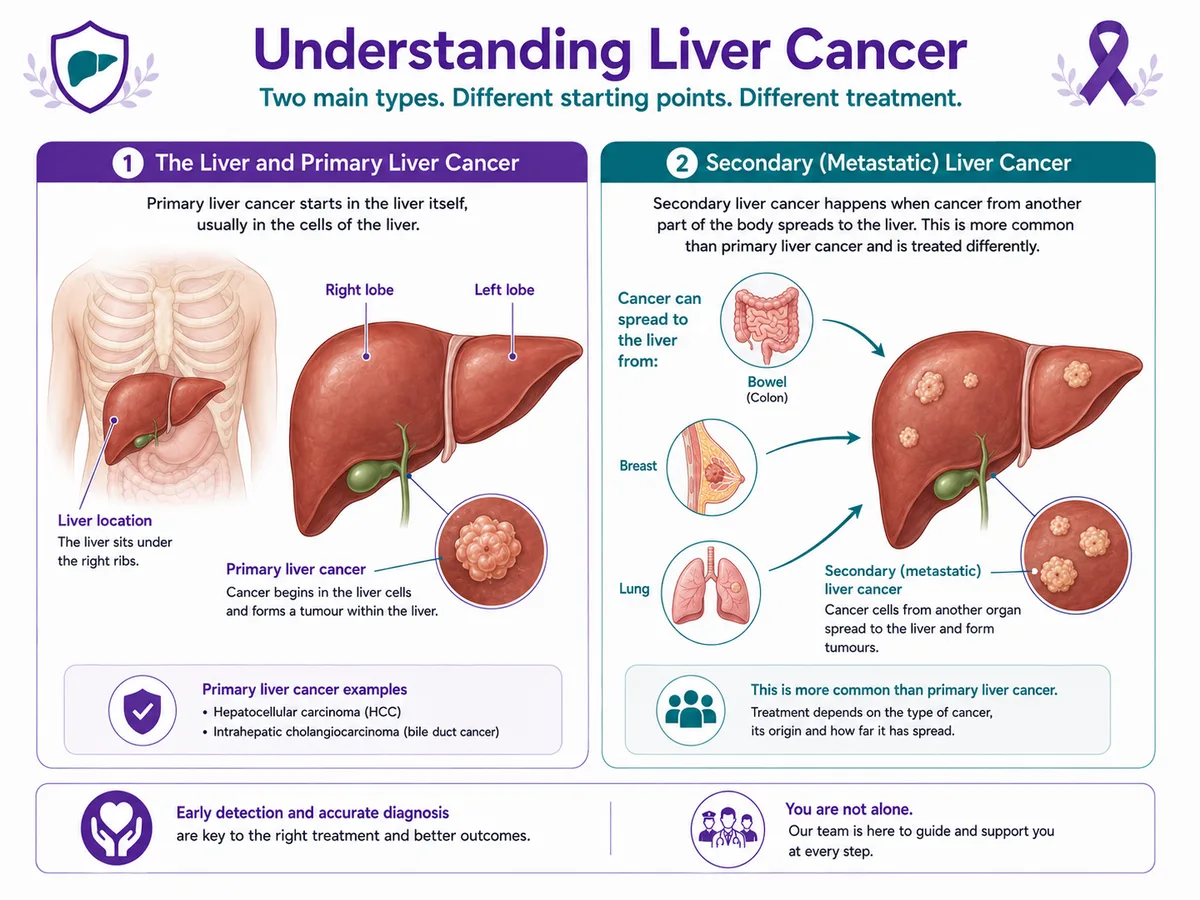
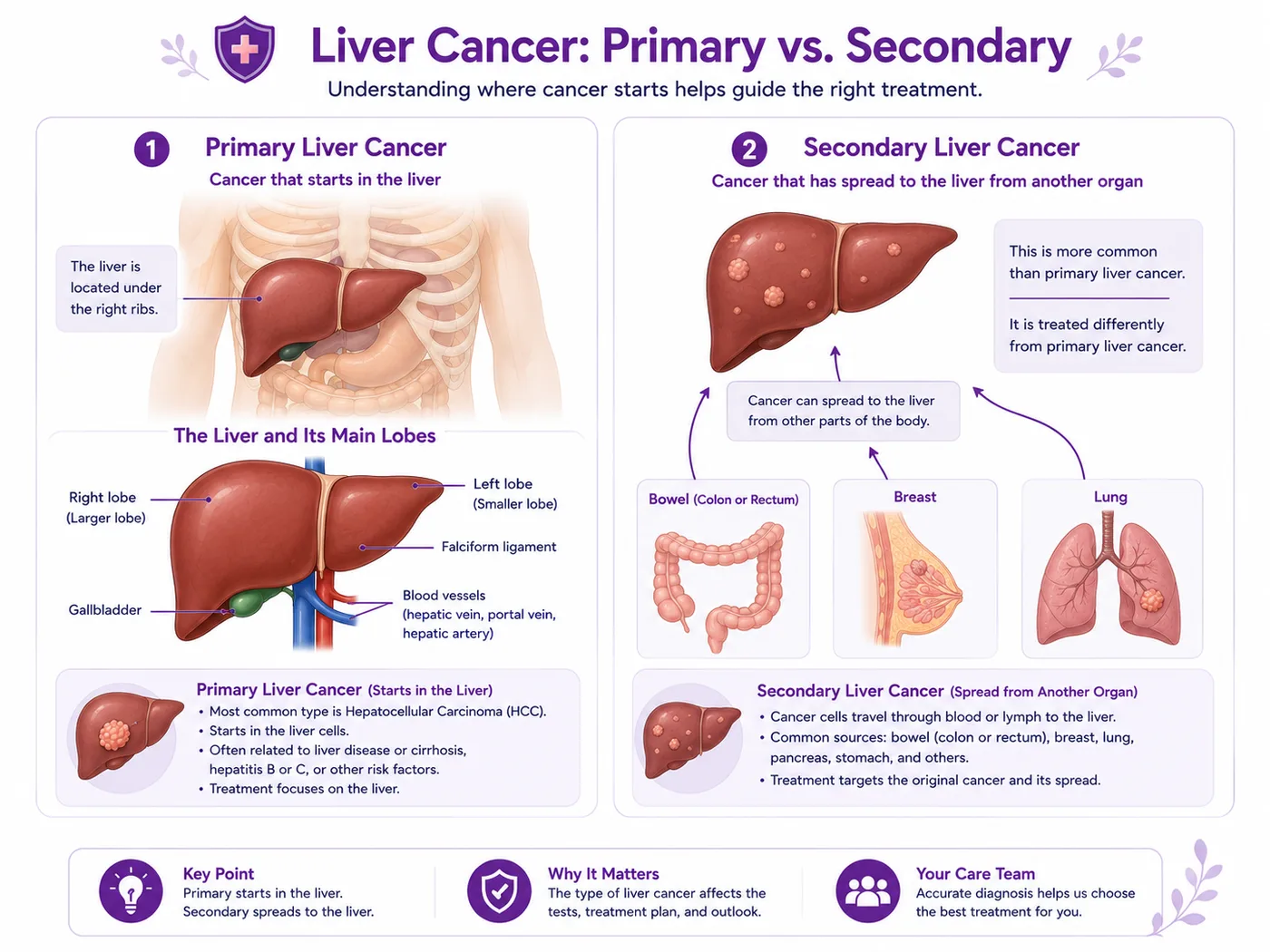
What is the difference between primary and secondary liver cancer?
Primary liver cancer starts in the liver itself. Secondary (or metastatic) liver cancer is cancer that spread to the liver from elsewhere — most often the bowel, but also the breast or lung — and is actually more common. They are treated very differently, so confirming which one it is is an essential first step.
What are the early symptoms of liver cancer?
Early liver cancer is usually silent, which is why it is so often found late without surveillance. As it grows, symptoms can include pain or a lump in the upper-right abdomen, jaundice (yellowing of the eyes and skin), abdominal swelling, loss of appetite or feeling full quickly, unexplained weight loss and tiredness. Because early disease causes no symptoms, people at risk should not wait for signs — surveillance is the safer route.
What is hepatocellular carcinoma (HCC)?
Hepatocellular carcinoma, or HCC, is the commonest type of primary liver cancer. It starts in the main cells of the liver (hepatocytes) and usually develops in a liver already damaged by long-term hepatitis B or C, cirrhosis or fatty liver. Because it grows on a background of liver disease, it is often silent early — and is exactly what 6-monthly surveillance in at-risk people aims to catch.
What causes liver cancer, and who is at higher risk?
Most liver cancer is caused by long-term liver damage. The main risk factors are chronic hepatitis B, chronic hepatitis C, cirrhosis (from any cause, including alcohol), heavy or long-term alcohol use, and fatty liver disease linked to obesity and type 2 diabetes; a family history and aflatoxin exposure also contribute. Having a risk factor does not mean you will get liver cancer — but it does mean testing and, where advised, surveillance are worthwhile.
Does the hepatitis B vaccine prevent liver cancer?
Yes — substantially. Because chronic hepatitis B is a leading cause of liver cancer, the hepatitis B vaccine is one of the few vaccines that helps prevent a cancer. It is safe and effective, protects against hepatitis B infection, and is given routinely to infants; unvaccinated adults, and especially close contacts of someone with hepatitis B, can also be vaccinated. It is a genuine, practical way to lower liver-cancer risk.
Can hepatitis C be cured, and does that lower my risk?
Yes. Modern tablet treatments can cure most hepatitis C infections in a few weeks, and clearing the virus lowers the risk of liver cancer and further liver damage. Hepatitis B is not usually cured but can be well controlled with treatment, which also reduces risk. The first step for both is a simple blood test — many people carry hepatitis B or C without knowing.
Can fatty liver lead to liver cancer?
It can, in some people. Fatty liver disease — linked to obesity, type 2 diabetes and metabolic syndrome — is becoming a more common cause of liver cancer in India. Most people with fatty liver will never develop cancer, but ongoing inflammation and cirrhosis raise the risk. Keeping to a healthy weight, controlling diabetes and limiting alcohol help protect the liver; a doctor can advise whether you need monitoring.
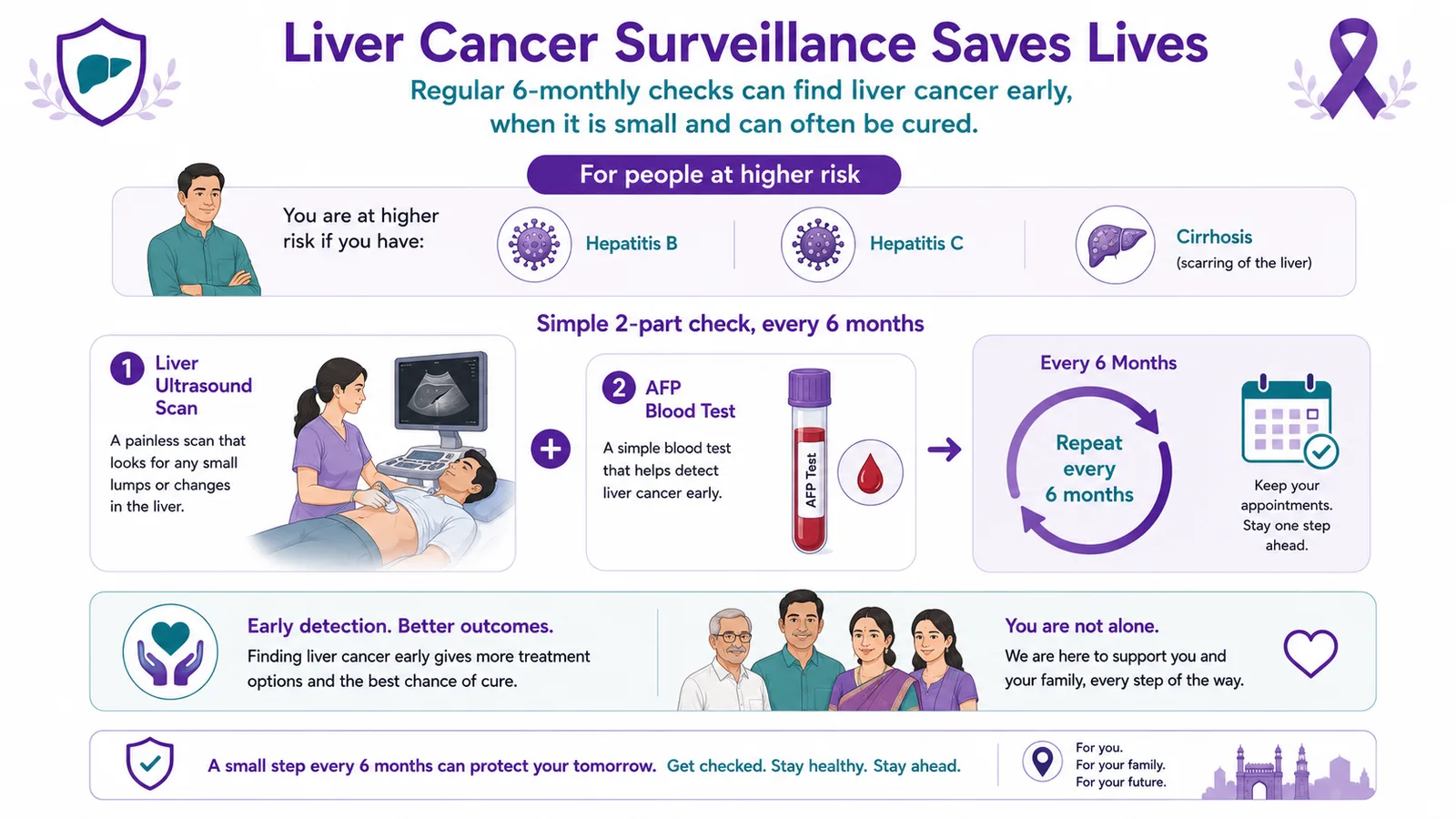
What is liver cancer surveillance, and who needs it?
Surveillance means regular checks — usually a liver ultrasound and an AFP blood test about every 6 months — for people at higher risk, such as those with hepatitis B, hepatitis C or cirrhosis. Because liver cancer is silent early, surveillance is the single most effective way to catch it while it is small and often curable. Not everyone with liver disease needs it; a doctor advises based on your liver health.
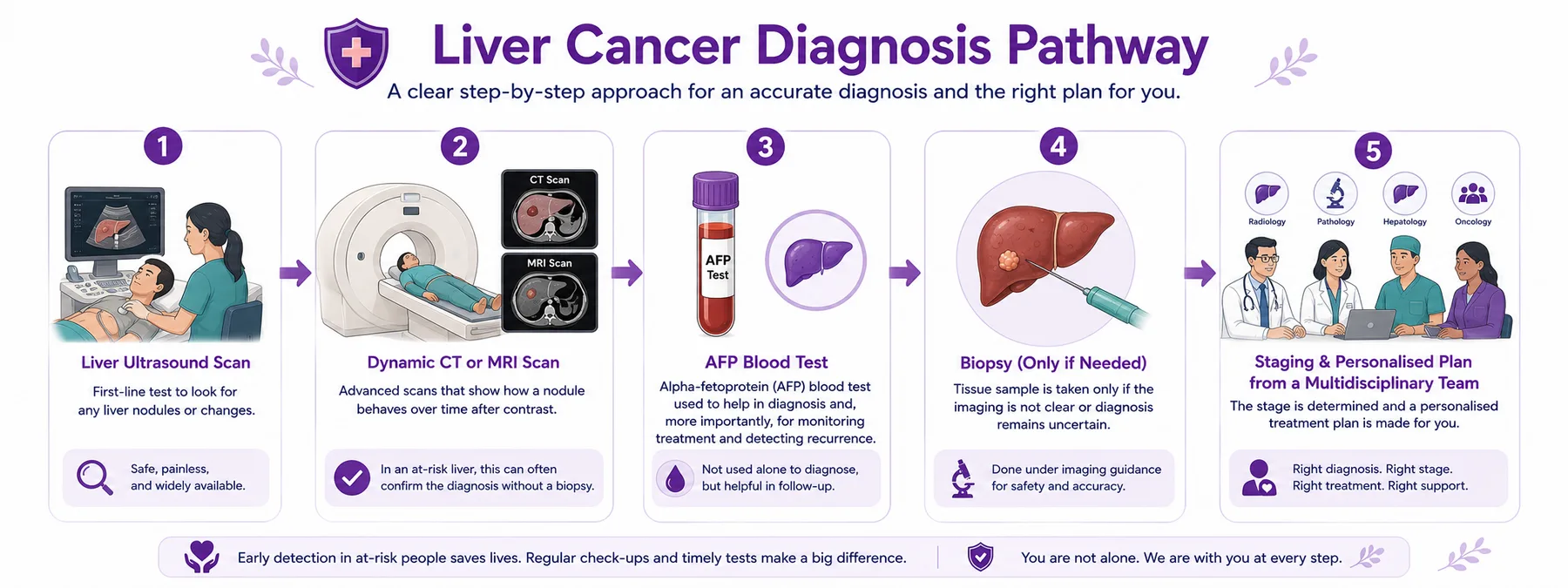
How is liver cancer diagnosed — do I always need a biopsy?
Often not. In a liver already at risk (from hepatitis or cirrhosis), characteristic findings on a dynamic contrast CT or MRI scan can confirm liver cancer without a biopsy. An ultrasound usually finds it first (often on surveillance), and an AFP blood test helps with monitoring. A biopsy is used only when the imaging is unclear or there is no known liver disease — it is a safe, standard step when it is needed.
What is an AFP blood test?
AFP (alpha-fetoprotein) is a protein that can be raised in the blood in some liver cancers. It is used mainly alongside ultrasound for surveillance, and to help monitor how treatment is working — not as a stand-alone diagnosis, because it can be normal in some liver cancers and raised by other liver conditions. Your doctor interprets it together with your scans.
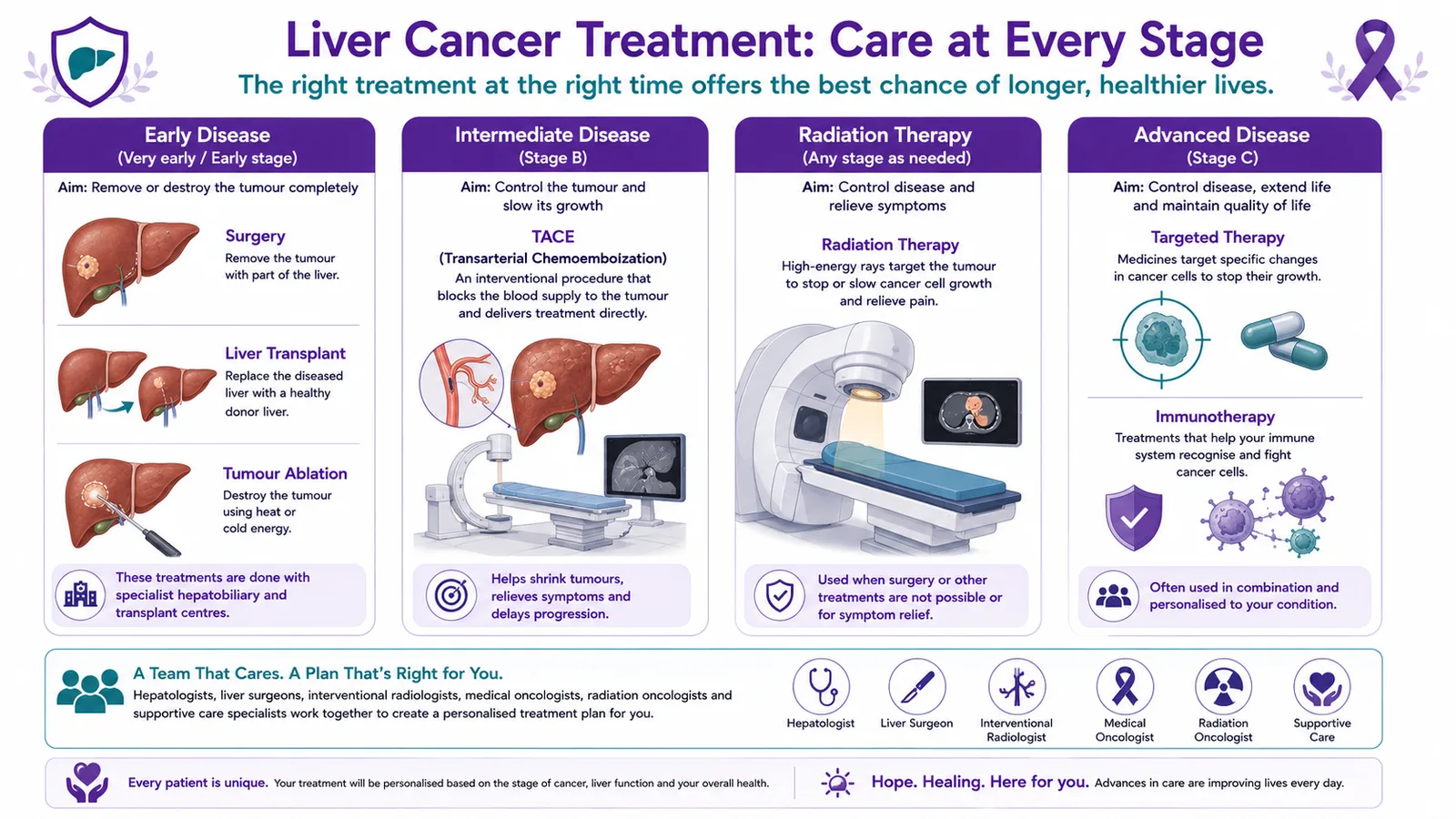
How is liver cancer staged?
Liver cancer is staged differently from most cancers, commonly using the BCLC system, which looks not only at the tumour but at how well the liver is working — because a healthy liver can tolerate treatments a damaged one cannot. Broadly, it ranges from very early and early (often curable with surgery, transplant or ablation), to intermediate (procedures such as TACE), advanced (systemic therapy), and end-stage (comfort-focused care).
What is TACE?
TACE (transarterial chemoembolisation) is a treatment mainly for intermediate-stage liver cancer that is still confined to the liver. Through a fine tube in a blood vessel, treatment is delivered directly to the tumour and its blood supply is blocked, which helps shrink it and slow its growth. It is an interventional radiology procedure, coordinated with specialist partners, and is often combined with other treatments.
Can a liver transplant treat liver cancer?
Yes — for selected early liver cancers, a liver transplant is one of the most curative options, because it removes both the cancer and the damaged liver that caused it. Whether a transplant is suitable depends on the size and number of tumours, the state of the liver, and overall health. At CION it is coordinated with specialist liver-transplant centres, as part of a plan managed by our team.
Is liver cancer curable?
It can be, especially when found early. A small liver cancer in a reasonably healthy liver can often be cured with surgery, a transplant or ablation — which is exactly what surveillance aims to catch. Even advanced liver cancer, once very hard to treat, is now often controlled for a long time with immunotherapy and targeted therapy. The outlook depends on the stage and on how well the liver is working, and is best judged by a specialist team.
How is advanced liver cancer treated?
Advanced liver cancer — which has spread within or beyond the liver — is treated mainly with systemic therapy: immunotherapy and targeted therapy, which have transformed what is possible and can control the disease, sometimes for a long time. Modern, precise radiation (SBRT) is used for selected tumours, and strong supportive care runs alongside to protect quality of life. The plan is decided by a multidisciplinary team and made with you.
How much does liver cancer treatment cost in Hyderabad?
It varies widely with the stage and treatment — and some treatments (a liver transplant, ablation or TACE) are delivered at specialist partner centres and may be billed there. It is best given as an indicative range after assessment. Eligible treatment may be covered under Aarogyasri or PMJAY at empanelled centres. Use the cost estimator on this page for an indicative figure, then request a callback for an accurate estimate.
Does liver cancer treatment qualify for Aarogyasri or PMJAY?
Eligible liver cancer treatment may be largely covered under Aarogyasri and PMJAY at empanelled centres, and cost should not delay care. Our team helps check your eligibility and guides you on private insurance and EMI options. Because some procedures (such as transplant, ablation or TACE) may be delivered at partner centres, we explain clearly what is covered and where, so there are no surprises.