Pancreatic Cancer: Facing It with Honesty — and Real Hope
Pancreatic cancer is a serious diagnosis, and often found late — we won’t pretend otherwise. But it isn’t hopeless: caught early, some tumours can be removed and cured; modern chemotherapy can sometimes make surgery possible; and expert supportive care protects how you live. The sign that matters most is jaundice — never ignore it.
Free consultation with a medical oncologist
Resectability review — can it be removed? — by a coordinated HPB/GI team
9 clinics in Hyderabad · 35+ across Telangana & AP
Written & medically reviewed by Dr. C. Raghavendra Reddy, Medical Oncologist (DM Medical Oncology, DNB), CION Cancer Clinics — with our radiation oncology team. · Reviewed 9 July 2026
Overview
What is pancreatic cancer?
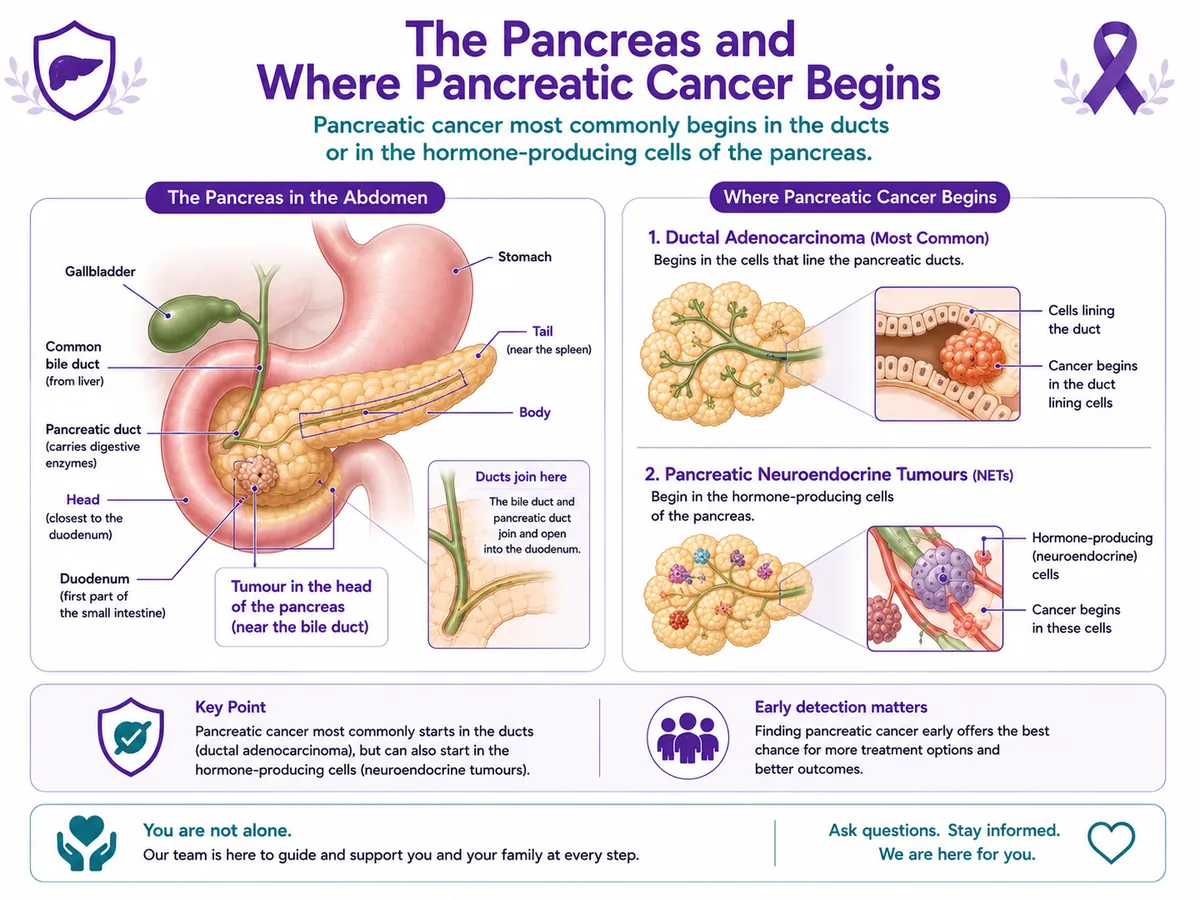
Pancreatic cancer begins when cells in the pancreas grow out of control. The commonest type, ductal adenocarcinoma, starts in the ducts and can be aggressive; a less common type, a neuroendocrine tumour, starts in hormone-producing cells and often behaves very differently, with a better outlook. Because the pancreas sits deep in the abdomen, early pancreatic cancer is often silent — which is why the warning signs below matter.
The pancreas sits behind the stomach. A tumour in its “head” lies close to the bile duct — which is why it can cause jaundice, sometimes relatively early.
The commonest pancreatic cancer starts in the ducts; a head tumour sits near the bile duct.
Jaundice matters most
Jaundice, or another warning sign? What it means
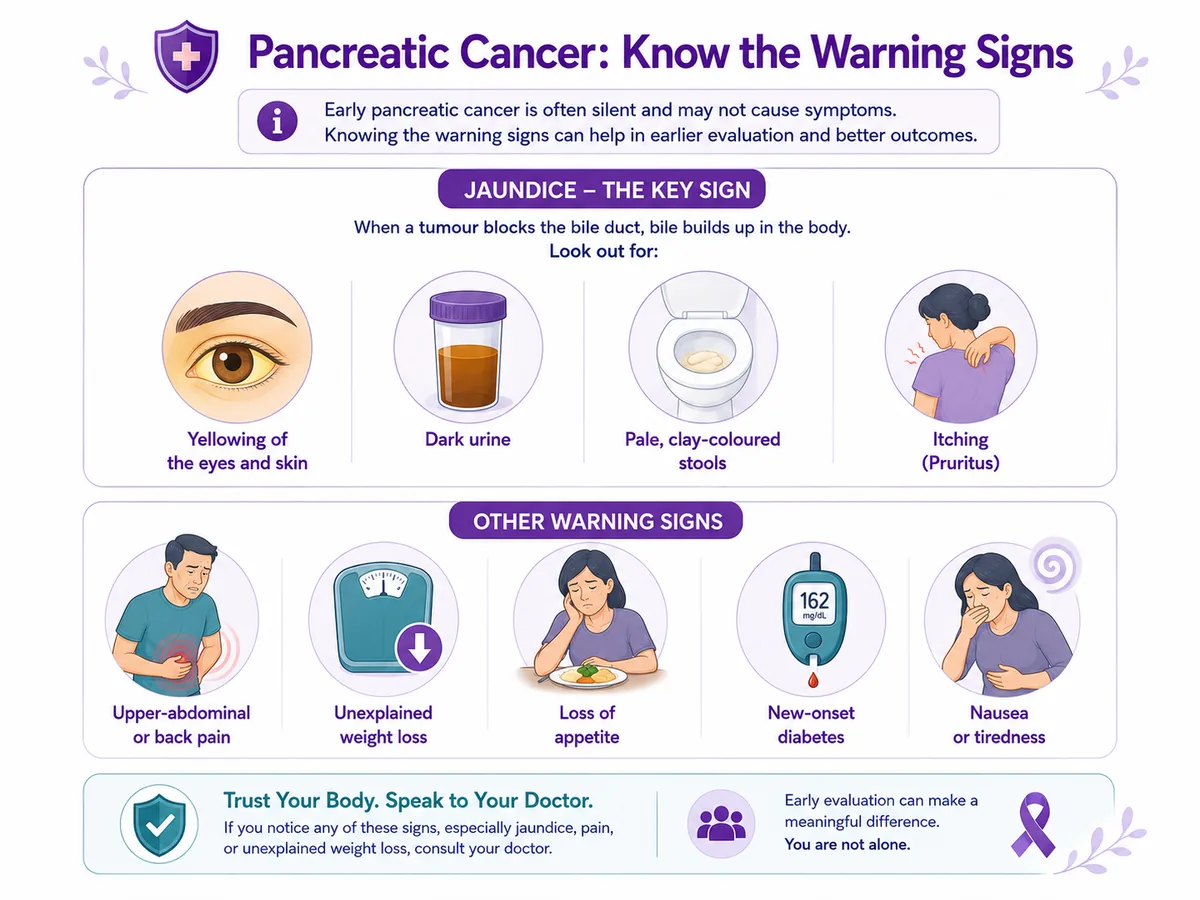
The sign that matters most is jaundice — yellowing of the eyes or skin, dark urine, pale stools, sometimes with itching. It has many causes, most not cancer, but it should always be checked urgently: when pancreatic cancer causes jaundice, it can sometimes be caught while still treatable.
Should I get this checked?
Tick anything that applies. This is an awareness guide, not a diagnosis.
Your result
Tick what applies
Most of these symptoms have causes other than cancer. Your guidance appears here.
This tool doesn’t diagnose anything or replace medical advice. Jaundice, or persistent pain, weight loss or new diabetes, should be checked by a doctor — most causes aren’t cancer, but prompt assessment matters.
Symptoms
Signs & symptoms
Early pancreatic cancer is often silent, and its symptoms can be vague. The most important is jaundice; others include upper-abdominal or back pain, unexplained weight loss, loss of appetite, new-onset diabetes, greasy pale stools, nausea and tiredness. Any of these that persist deserve checking.
Jaundice (yellow eyes/skin, dark urine)
Upper-tummy or back pain
Unexplained weight loss
Loss of appetite
New-onset diabetes
Greasy pale stools, nausea
Painless jaundice — or persistent symptoms lasting more than a couple of weeks — is the pattern that matters. If that’s you, book a consultation.
Early clues
Early clues worth acting on
Two clues are worth knowing about — neither means cancer, but both are worth mentioning to your doctor. First, new diabetes appearing in an older adult, especially alongside unexplained weight loss rather than weight gain. Second, persistent upper-abdominal or back pain together with weight loss. Most often these have other explanations — but occasionally they’re an early sign, and asking costs nothing.
New diabetes in an older adult
The vast majority of new diabetes is ordinary type 2 — but new diabetes with weight loss (not weight gain) in an older adult is occasionally an early clue worth mentioning.
Back pain + weight loss
Persistent upper-abdominal or back pain, together with unexplained weight loss, is worth getting checked — most causes aren’t cancer, but it shouldn’t be ignored.
Causes & risk
Causes & risk factors
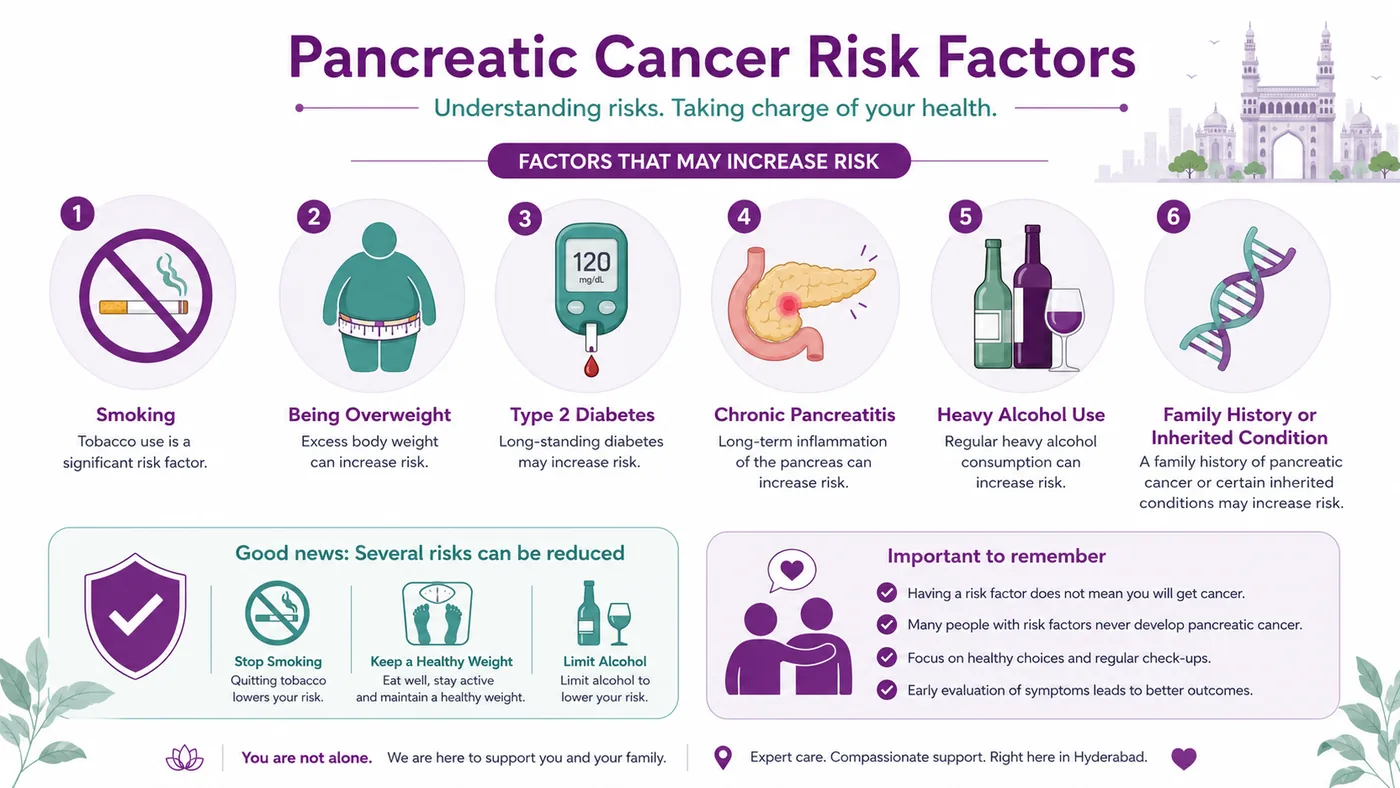
Pancreatic cancer doesn’t have a single cause, but several things raise the risk — and several are within your control. Smoking is the biggest modifiable risk; being overweight, heavy alcohol, chronic pancreatitis and long-standing diabetes also contribute, and some people carry an inherited risk (a family history, or conditions linked to genes like BRCA and Lynch syndrome). Having a risk factor doesn’t mean you’ll get pancreatic cancer.
Most pancreatic cancers are ductal adenocarcinoma, which starts in the ducts and tends to be aggressive. A much less common group, neuroendocrine tumours, start in hormone-producing cells, often grow more slowly, and generally have a better outlook — and are treated quite differently.
Understand the types
Simplified for understanding. Your exact type is confirmed by your team and guides your personalised plan.
Staging
The stages of pancreatic cancer
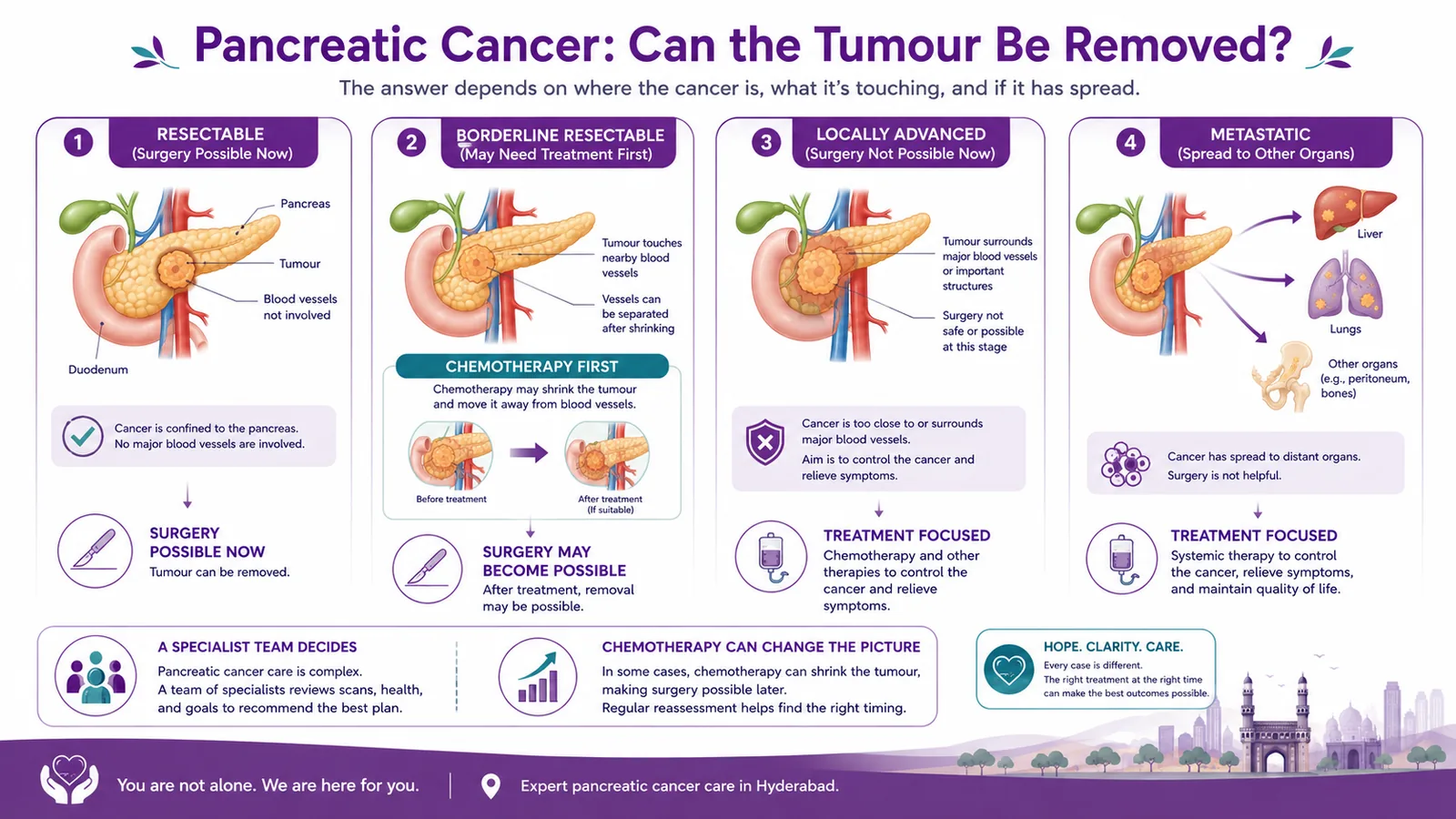
Pancreatic cancer is grouped less by a simple number and more by one crucial question: can it be removed by surgery? Doctors classify it as resectable, borderline resectable, locally advanced, or metastatic — based on whether it has spread and how it relates to nearby blood vessels.
Understand the stages
Simplified for understanding. Whether surgery is possible is decided by a specialist team after tests.
Diagnosis
How pancreatic cancer is diagnosed
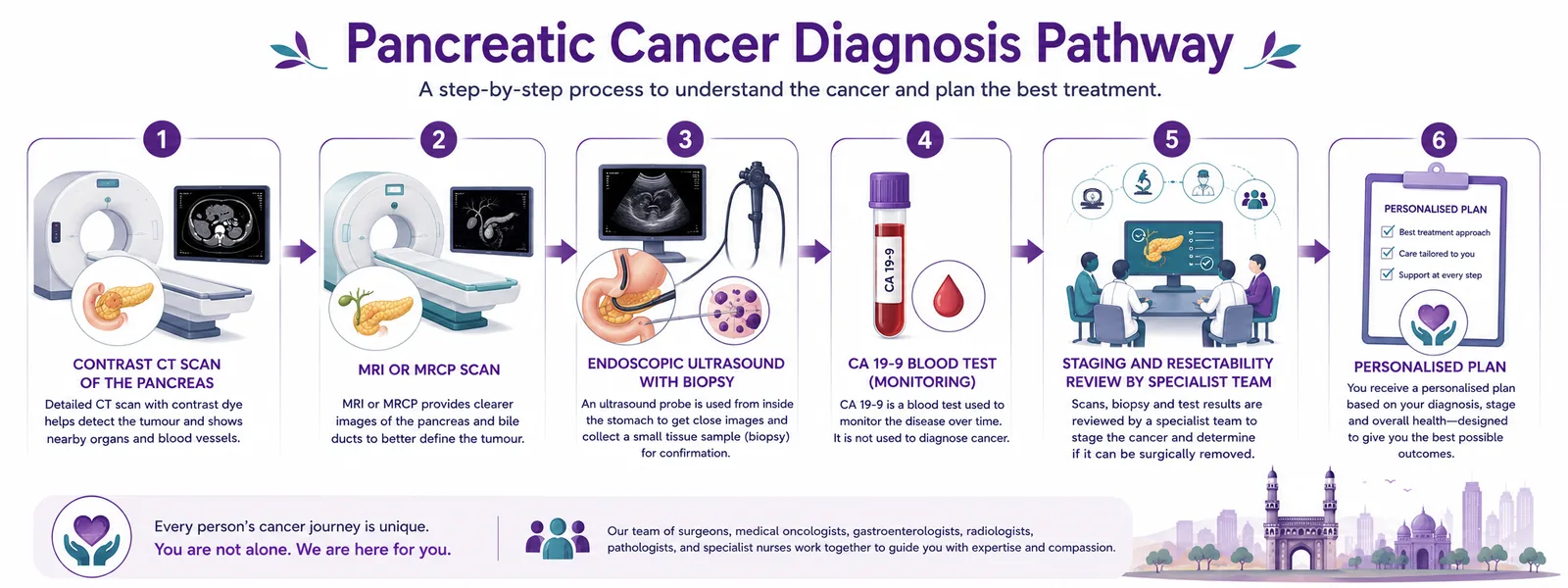
Pancreatic cancer is diagnosed with a contrast CT scan, often with an MRI or MRCP, and an endoscopic ultrasound that allows a small tissue sample (biopsy) to be taken. A blood marker called CA 19-9 helps with monitoring rather than diagnosis. A specialist team then reviews whether the tumour can be removed. Because symptoms appear late, prompt assessment matters.
From scans and a biopsy to a specialist team decision on whether surgery is possible.
Diagnostic services we offer — book any of these directly:
Contrast CT scan
The first-line scan for the pancreas — it maps the tumour and its relationship to nearby blood vessels.
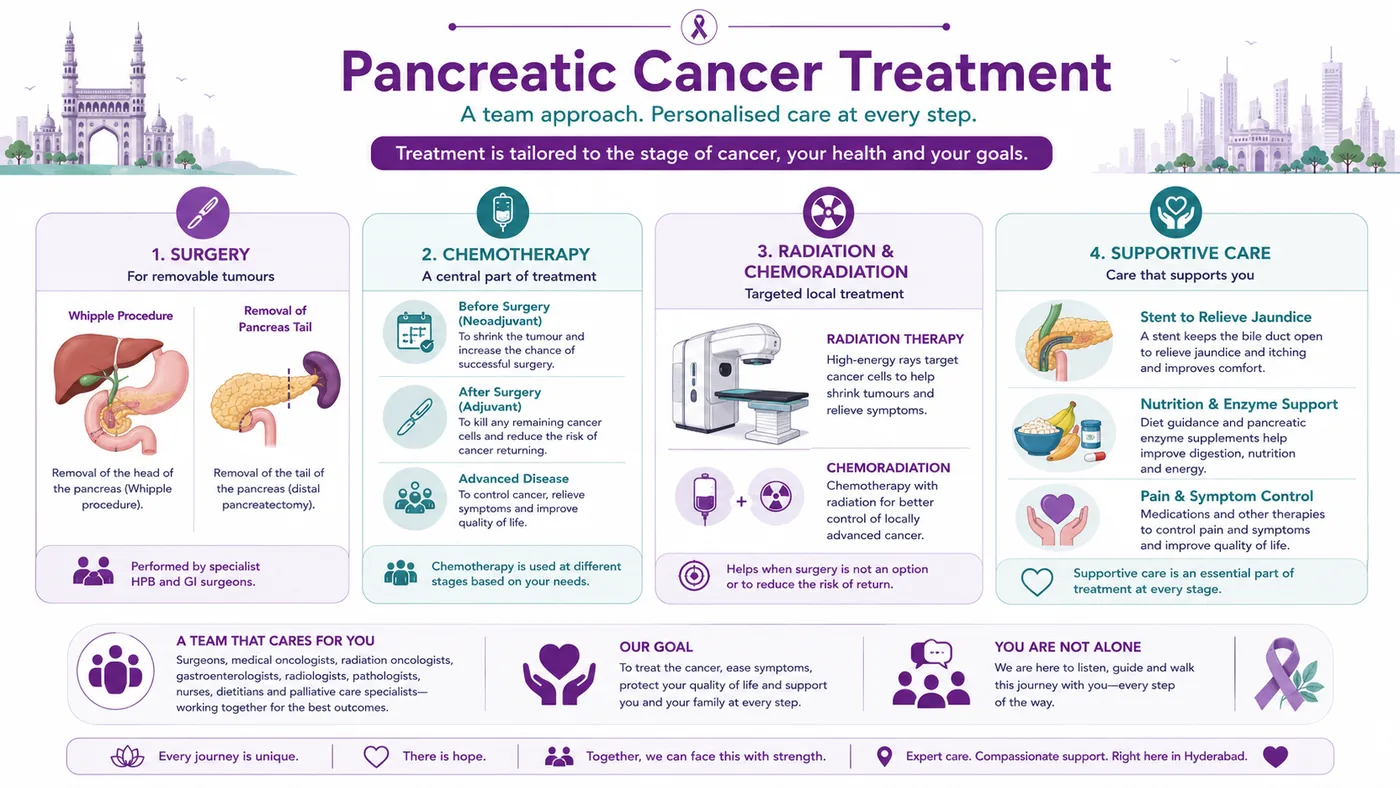
Pancreatic cancer is treated by a multidisciplinary team, and the plan depends on whether surgery is possible. For removable tumours, surgery followed by chemotherapy offers the best chance of cure. Chemotherapy is central throughout — before surgery, after surgery, and as the main treatment for advanced disease — with radiation in some cases. And supportive care, to relieve jaundice and protect nutrition and comfort, is a core part of treatment, not an afterthought. See our full guide to pancreatic cancer treatment in Hyderabad.
A coordinated team. CION provides medical oncology (chemotherapy) and radiation in-house, and works with specialist HPB/GI surgeons, gastroenterology and endoscopy for pancreatic surgery and biliary stenting — so your whole pathway is planned and managed together.
Treatments & care we coordinate — book a consult for any of these:
Surgery — Whipple / distal (coordinated)
The Whipple procedure or removal of the pancreas tail, for removable tumours — coordinated with specialist HPB/GI surgeons.
The single biggest question in pancreatic cancer is whether the tumour can be removed by surgery — and the answer isn’t always a simple yes or no. Some tumours are removable straight away. Others, called “borderline,” touch nearby blood vessels — but chemotherapy given first can sometimes shrink them enough to make surgery possible. This is why a specialist team assessment (and often a second opinion) matters so much: the door to surgery is sometimes wider than it first appears.
Indicative cost of pancreatic cancer treatment in Hyderabad
Cost varies widely with the stage and treatment — and some treatments (pancreatic surgery or biliary stenting) are delivered at specialist partner centres and may be billed there. It’s best given as an indicative range after assessment. Eligible treatment may be covered under Aarogyasri / PMJAY at empanelled centres.
Estimate an indicative range
Indicative range
—
Figures are indicative only and not a quotation — pancreatic surgery and biliary stenting may be delivered and billed at specialist partner centres. For an accurate estimate, request a callback.
Jaundice, unexplained weight loss, a scan finding, or a diagnosis you want a second view on shouldn’t wait. Book a free consultation and, if you already have a report, a free written second opinion — including whether surgery is possible.
Reviewed by a medical oncologist and an HPB tumour board
Resectability review — can it be removed? — and downstaging options
Aarogyasri / PMJAY & insurance guidance
Support
Financial support & Aarogyasri
Cost should not delay care. Under Aarogyasri and PMJAY, eligible pancreatic cancer treatment may be largely covered at empanelled centres. Our team helps check eligibility and guides you on insurance and EMI.
9 clinics in Hyderabad · 35+ across Telangana & AP
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the oncologists
Pancreatic cancer is treated by a team, not one doctor.
Care is led by medical oncology (chemotherapy is central here), with radiation oncology in-house and a coordinated HPB/GI surgical and endoscopy team — part of 17 senior specialists across CION.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Yellow eyes or skin? Don’t wait — get jaundice checked.
Painless jaundice, unexplained weight loss or persistent back pain deserve prompt assessment — and if you’ve been diagnosed, whether surgery is possible is best decided by a specialist team. Our oncologists coordinate this every day.
The worries and myths we hear most about pancreatic cancer, answered honestly.
“Pancreatic cancer is always a death sentence.”
Fact: It’s serious and often found late — but not hopeless. Early tumours can be cured by surgery, chemo can downstage some, neuroendocrine tumours fare better, and supportive care protects quality of life.
“Yellow eyes are just a jaundice problem, not urgent.”
Fact: Painless jaundice always needs urgent assessment — and if it’s pancreatic cancer, it can be a sign caught while still treatable.
“New diabetes means I have pancreatic cancer.”
Fact: Almost all new diabetes is ordinary type 2 — but new diabetes with weight loss in an older adult is occasionally a clue worth mentioning.
“If it can’t be removed now, nothing can be done.”
Fact: Chemotherapy can sometimes make a borderline tumour operable, and can control disease and symptoms even when surgery isn’t possible.
“Treatment will destroy my quality of life.”
Fact: Supportive care — a stent for jaundice, nutrition and enzyme support, modern pain control — is central, helping people feel as well as possible.
“There’s no point getting a second opinion.”
Fact: Whether surgery is possible can differ between assessments — a specialist opinion at a centre that treats pancreatic cancer genuinely matters.
“Pancreatic cancer always causes severe pain from the start.”
Fact: Early disease is often painless or vague — that’s why subtle signs like jaundice, weight loss and new diabetes matter more than waiting for pain.
“A biopsy or surgery will make the cancer spread.”
Fact: Diagnosis and surgery are safe, standard steps done under controlled conditions. The real risk is delay, which lets a treatable cancer grow.
“Cancer is contagious — I could catch it from someone.”
Fact: Pancreatic cancer is not infectious. You can’t catch it by living with, caring for or being close to someone who has it.
“Only heavy drinkers and smokers get pancreatic cancer.”
Fact: Smoking is the biggest modifiable risk, but many people with pancreatic cancer never smoked or drank heavily — age, diabetes, pancreatitis and family history all play a part.
“Chemotherapy won’t help pancreatic cancer.”
Fact: Chemotherapy is the backbone of pancreatic cancer care — before surgery, after surgery, and for advanced disease — and can shrink some tumours enough to operate.
“The Whipple operation is too dangerous to consider.”
Fact: In experienced specialist hands it is a well-established operation that offers the best chance of cure for a removable head tumour — CION coordinates it with expert HPB/GI surgeons.
“Treatment is unaffordable — we can’t manage it.”
Fact: Under Aarogyasri and PMJAY, eligible treatment may be largely covered at empanelled centres. We help check eligibility, insurance and EMI.
“If it runs in my family, there’s nothing I can do.”
Fact: A family history can point to inherited risk (like BRCA or Lynch). Genetic counselling can clarify it — and, where relevant, open up monitoring and preventive options.
“Losing weight without trying is a good thing.”
Fact: Unexplained weight loss — especially with jaundice, tummy or back pain, or new diabetes — is worth checking. Most causes aren’t cancer, but it shouldn’t be ignored.
“Home remedies or diet alone can cure it.”
Fact: Relying on unproven remedies wastes the window when pancreatic cancer is most treatable. Discuss anything complementary with your oncology team, not as a replacement.
“Once pancreatic cancer comes back, there’s no point treating it.”
Fact: Even when it returns, further chemotherapy and strong supportive care can control the disease and protect how you live — treatment decisions are made with you.
“A cyst on my pancreas means I have cancer.”
Fact: Most pancreatic cysts are benign. Some types need monitoring or removal, so they’re assessed with scans — but a cyst is not the same as cancer.
Why CION
Why choose CION for pancreatic cancer care
Chemotherapy expertise
Chemotherapy is central to pancreatic cancer — before surgery, after surgery, and for advanced disease — led by medical oncology.
Coordinated HPB/GI pathway
The Whipple procedure, distal pancreatectomy and biliary stenting via specialist HPB/GI surgeons, gastroenterology and endoscopy — planned together.
Resectability-focused review
A specialist team assesses whether surgery is possible — and whether chemotherapy could make a borderline tumour operable.
Strong supportive care
Jaundice relief, nutrition and pancreatic enzyme support, and modern pain control — protecting quality of life throughout.
HPB tumour board
Every case discussed by a multidisciplinary team, matching treatment to the tumour and to you.
Close, NABH-accredited care
9 clinics across Hyderabad and 35+ across Telangana, within NABH-accredited facilities.
Real stories · real courage
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
In pancreatic cancer, supportive care is central — jaundice relief, nutrition, symptom control, wellbeing and family risk.
Nutrition & enzyme support
Diet guidance and pancreatic enzyme support to aid digestion and protect weight. Learn more
Pain & symptom relief
Modern pain control and relief of jaundice and other symptoms, at any stage. Learn more
Psycho-oncology
Emotional support for you and your family through a difficult diagnosis. Learn more
Genetic counselling
If pancreatic cancer runs in your family, advice on inherited risk (BRCA, Lynch) and testing. Learn more
Rehabilitation & recovery
Support to regain strength and wellbeing after surgery or treatment. Learn more
Second opinion
A clear, unhurried review of your diagnosis and whether surgery is possible. Get a second opinion
FAQ
Frequently asked questions about pancreatic cancer
Is pancreatic cancer always a death sentence?
No — although it is a serious cancer that is often found late, and it would be wrong to pretend otherwise, it is not hopeless. When it is found early and can be removed by surgery, some people are cured; chemotherapy can sometimes shrink a borderline tumour enough to operate; neuroendocrine tumours often do much better; and even when cure is not possible, treatment and supportive care can control the disease and protect quality of life. A specialist assessment is the best guide to your situation.
My eyes and skin have gone yellow — should I worry?
Jaundice — yellowing of the eyes or skin, dark urine, pale stools, sometimes with itching — should always be checked promptly. It has many causes, most not cancer, but it needs urgent assessment. If it is pancreatic cancer, jaundice can appear relatively early (from a tumour blocking the bile duct), which sometimes means it is caught while still treatable — and the jaundice itself can be relieved with a stent.
I have just been diagnosed with diabetes — could it be pancreatic cancer?
Almost always, no — the vast majority of new diabetes is ordinary type 2 diabetes, not cancer. But new diabetes in an older adult, especially alongside unexplained weight loss rather than weight gain, is occasionally an early clue, so it is worth mentioning any other symptoms to your doctor. Do not panic — but do not ignore weight loss.
What are the early symptoms of pancreatic cancer?
Early pancreatic cancer is often silent, and its symptoms can be vague. The most important is jaundice (yellow eyes or skin, dark urine, pale stools). Others include upper-abdominal or back pain, unexplained weight loss, loss of appetite, new-onset diabetes, greasy pale stools, nausea and tiredness. None of these mean cancer on their own — but any that are new and persist for more than a couple of weeks deserve checking.
Can pancreatic cancer be operated on?
It depends on whether the tumour can be removed — which is decided by its size, its spread, and its relationship to nearby blood vessels. Some are removable straight away; some borderline tumours can be made removable with chemotherapy first; and some cannot be operated on. A specialist team makes this assessment, which is why a second opinion at a centre that treats pancreatic cancer is worthwhile.
What is the Whipple procedure?
It is the main operation for a tumour in the head of the pancreas — removing the head of the pancreas along with parts of nearby organs, then reconnecting the digestive system. It is major surgery done by specialist hepatobiliary and GI surgeons, which is why CION coordinates it with expert surgical partners while managing your chemotherapy and overall care.
What does "resectable", "borderline" or "locally advanced" mean?
These describe whether a tumour can be removed. Resectable means it can be removed by surgery now. Borderline resectable means it touches nearby blood vessels, so chemotherapy (sometimes with radiation) is usually given first to try to shrink it into the operable group. Locally advanced means it involves major vessels and cannot be removed at present, though treatment can still control it. Metastatic means it has spread to distant organs, where treatment focuses on control and quality of life.
Can chemotherapy make surgery possible (downstaging)?
Sometimes, yes. For a borderline tumour that touches nearby blood vessels, chemotherapy given first — occasionally with radiation — can shrink it enough to move it into the removable group. This is called downstaging, and it is one of the most hopeful ideas in pancreatic cancer care. It is why a resectability review by a specialist team, and often a second opinion, is so valuable.
What are the types of pancreatic cancer?
Most pancreatic cancers are ductal adenocarcinoma (PDAC), which starts in the ducts of the pancreas and tends to be aggressive. A much less common group, pancreatic neuroendocrine tumours (pNETs), start in hormone-producing cells, often grow more slowly, and generally have a better outlook — and are treated quite differently. Your exact type is confirmed on a biopsy and guides your plan.
What is a pancreatic neuroendocrine tumour (pNET)?
A pNET is an uncommon type of pancreatic cancer that begins in the hormone-producing cells of the pancreas, rather than the ducts. pNETs often grow more slowly than adenocarcinoma and generally have a better outlook. Some are found because they produce hormones; others are found incidentally. They are treated quite differently, so confirming the type is an important first step.
What causes pancreatic cancer, and who is at higher risk?
Pancreatic cancer does not have a single cause. Smoking is the biggest modifiable risk; being overweight, heavy alcohol, chronic pancreatitis and long-standing type 2 diabetes also contribute. Older age raises risk, and some people carry an inherited risk through a family history or gene changes such as BRCA or Lynch syndrome. Having a risk factor does not mean you will get pancreatic cancer — and stopping smoking is one of the most useful steps you can take.
Is pancreatic cancer hereditary?
Most pancreatic cancer is not inherited, but a minority is linked to a family history or an inherited gene change such as BRCA1, BRCA2 or Lynch syndrome. If pancreatic cancer — or related cancers like breast, ovarian or bowel cancer — runs in your family, genetic counselling can clarify your risk and, where relevant, guide monitoring for close relatives. Everyone’s situation is different, so it is worth discussing with a specialist.
How is pancreatic cancer diagnosed?
It usually starts with a contrast CT scan, often followed by an MRI or MRCP, and an endoscopic ultrasound that allows a small tissue sample (biopsy) to be taken to confirm the diagnosis. A blood marker called CA 19-9 is used mainly to help monitor treatment rather than to diagnose. A specialist team then reviews all of this to decide whether the tumour can be removed. Because symptoms appear late, prompt assessment matters.
What is CA 19-9?
CA 19-9 is a protein that can be raised in the blood in pancreatic cancer. It is useful mainly for monitoring how treatment is working, not as a stand-alone screening or diagnostic test — it can be normal in some pancreatic cancers and raised by harmless conditions such as gallstones or a blocked bile duct. Your doctor interprets it alongside your scans and biopsy.
How is jaundice treated in pancreatic cancer?
When a tumour blocks the bile duct and causes jaundice, a small tube called a stent can be placed to reopen the duct and relieve the yellowing, itching and other symptoms. This is done via a coordinated endoscopy procedure and is often one of the first, most helpful steps — it can make you feel much better and help you tolerate other treatment. It is arranged with our gastroenterology and endoscopy partners.
How is pancreatic cancer treated?
Treatment is planned by a multidisciplinary team and depends on whether surgery is possible. For removable tumours, surgery (the Whipple procedure or distal pancreatectomy, coordinated with specialist HPB/GI surgeons) followed by chemotherapy offers the best chance of cure. Chemotherapy is central throughout — before surgery, after surgery, and as the main treatment for advanced disease — with radiation in selected cases. Supportive care, including jaundice relief and nutrition, runs alongside from the start.
Is pancreatic cancer curable?
It can be, particularly when it is found early and can be removed by surgery, usually followed by chemotherapy. It is often found late, which makes cure harder — but even then, treatment can control the disease, relieve symptoms and protect quality of life, and chemotherapy can sometimes make surgery possible in borderline cases. Neuroendocrine tumours generally have a better outlook. A specialist assessment is the best guide to what is possible for you.
How much does pancreatic cancer treatment cost in Hyderabad?
It varies widely with the stage and treatment — and some treatments (pancreatic surgery or biliary stenting) are delivered at specialist partner centres and may be billed there. It is best given as an indicative range after assessment. Eligible treatment may be covered under Aarogyasri or PMJAY at empanelled centres. Use the cost estimator on this page for an indicative figure, then request a callback for an accurate estimate.
Does pancreatic cancer treatment qualify for Aarogyasri or PMJAY?
Eligible pancreatic cancer treatment may be largely covered under Aarogyasri and PMJAY at empanelled centres, and cost should not delay care. Our team helps check your eligibility and guides you on private insurance and EMI options. Because some procedures may be delivered at partner centres, we will explain clearly what is covered and where, so there are no surprises.
Can pancreatic cancer be prevented or the risk reduced?
There is no guaranteed way to prevent pancreatic cancer, but you can lower your risk. Stopping smoking is the single most useful step, as smoking is the biggest modifiable risk factor. Keeping to a healthy weight, limiting alcohol, and managing diabetes also help. For people with a strong family history or a known inherited gene change, genetic counselling can advise on monitoring. Knowing the warning signs — especially jaundice — helps with earlier assessment.
Explore
Explore pancreatic & HPB cancer care
Our guide to pancreatic cancer — treatment, doctors, the resectability question, tests and support — plus the wider hepato-pancreato-biliary (HPB) cluster. Tap any topic to read more.
A pancreatic cancer diagnosis — or worrying symptoms? Talk to a specialist.
Jaundice, unexplained weight loss, or persistent back pain deserve prompt assessment — and if you’ve been diagnosed, whether surgery is possible is best decided by a specialist team. Book a consultation or second opinion at any of our 9 Hyderabad clinics, part of 35+ centres across Telangana & Andhra Pradesh.
Medical disclaimer: This page is for general information and awareness and does not replace professional medical advice, diagnosis or treatment. New jaundice (yellow eyes or skin), severe abdominal pain, or vomiting needs prompt medical attention. Always consult a qualified oncologist or gastroenterologist. Costs shown are indicative only and not a quotation. Content is periodically reviewed by CION’s medical team.