Ovarian cancer is often called a “silent killer” — but that’s not quite true. It does cause symptoms: persistent bloating, feeling full quickly and pelvic pain. Knowing them, knowing your family’s BRCA risk, and acting early make a real difference — and even advanced ovarian cancer responds well to treatment.
Free consultation with a medical oncologist
Genetic counselling & BRCA testing — for you and your family
9 clinics in Hyderabad · 35+ across Telangana & AP
Written & medically reviewed by Dr. C. Raghavendra Reddy, Medical Oncologist (MBBS, DM Medical Oncology, DNB), CION Cancer Clinics — with our radiation oncology team. · Reviewed 9 July 2026
Overview
What is ovarian cancer?
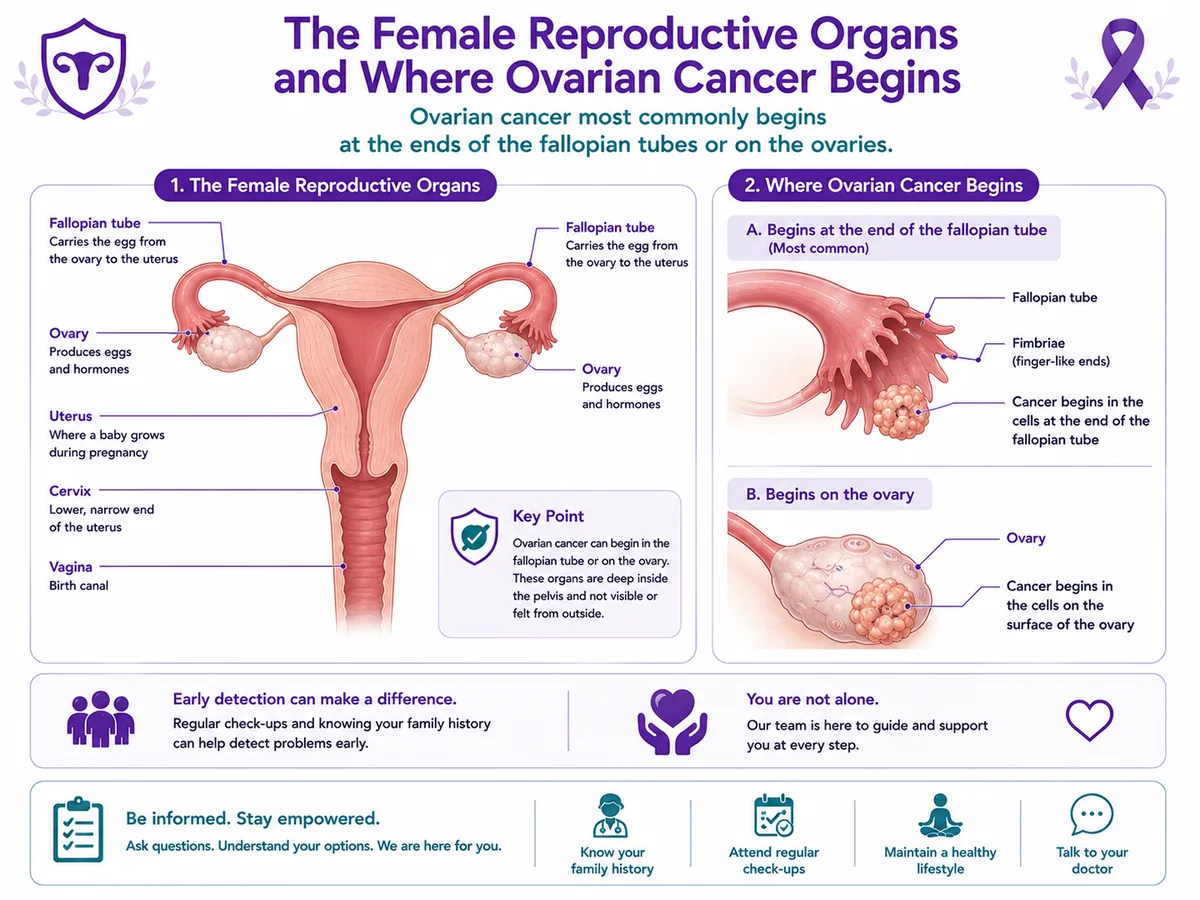
Ovarian cancer begins when cells in the ovaries — or, as we now know, often the fallopian tubes — grow out of control. The commonest type, high-grade serous carcinoma, is a form of “epithelial” ovarian cancer; a separate group, germ cell tumours, mostly affect younger women and are usually very treatable. Because the ovaries sit deep in the pelvis, ovarian cancer can grow quietly — but, as the next section explains, it’s not truly silent.
A woman has two ovaries, one each side of the uterus, with a fallopian tube alongside. Many high-grade serous cancers are now thought to start at the end of the fallopian tube.
The ovaries, fallopian tubes and uterus — where ovarian cancer begins.
Not silent
Bloating or another symptom? What it means
Ovarian cancer has been called a “silent killer,” but that’s not quite right: it does cause symptoms — they’re just subtle and easy to put down to something else. The ones that matter are persistent bloating, feeling full quickly, pelvic or tummy pain, and needing to pass urine urgently or often. What counts is whether they’re new, happen most days, and don’t settle.
Should I get this checked?
Tick anything that applies. This is an awareness guide, not a diagnosis.
Your result
Tick what applies
Occasional bloating or discomfort is very common and usually not cancer. Your guidance appears here.
This tool doesn’t diagnose anything or replace medical advice. New symptoms that happen most days for a few weeks should be checked by a doctor — most turn out to be harmless, and catching ovarian cancer sooner makes a real difference.
Symptoms
Signs & symptoms
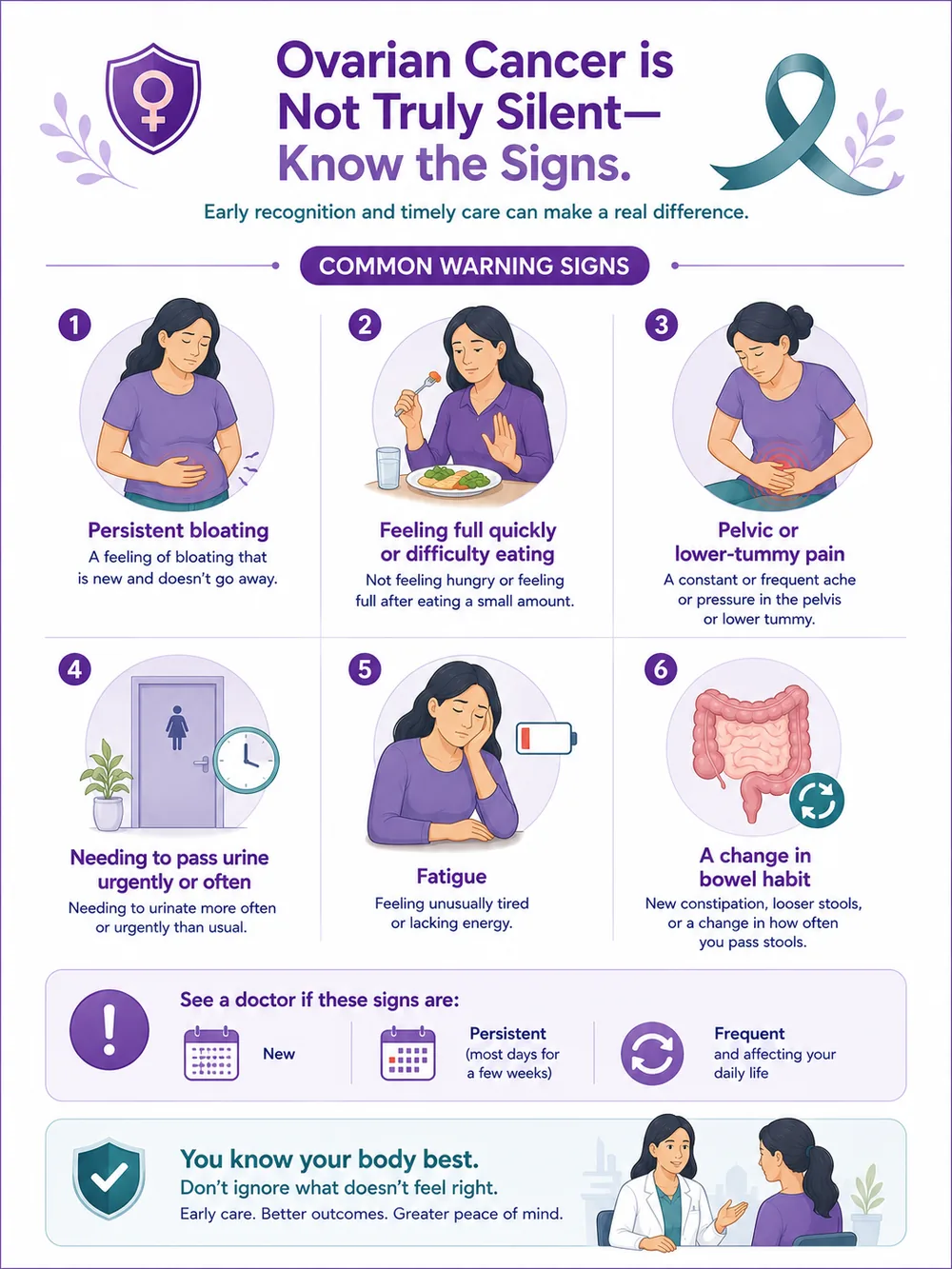
The key point about ovarian cancer symptoms is not that they’re absent, but that they’re vague. The four that matter most are persistent bloating, feeling full quickly (or difficulty eating), pelvic or tummy pain, and urinary urgency or frequency. Fatigue, a change in bowel habit and back pain can also occur. See a doctor if these are new, persist most days, and are frequent.
Persistent bloating
Feeling full quickly / difficulty eating
Pelvic or tummy pain
Urinary urgency or frequency
Fatigue
Change in bowel habit
New, persistent and frequent is the pattern that matters. If that’s you — especially with a family history of ovarian or breast cancer — book a consultation.
Causes & risk
Causes & risk factors
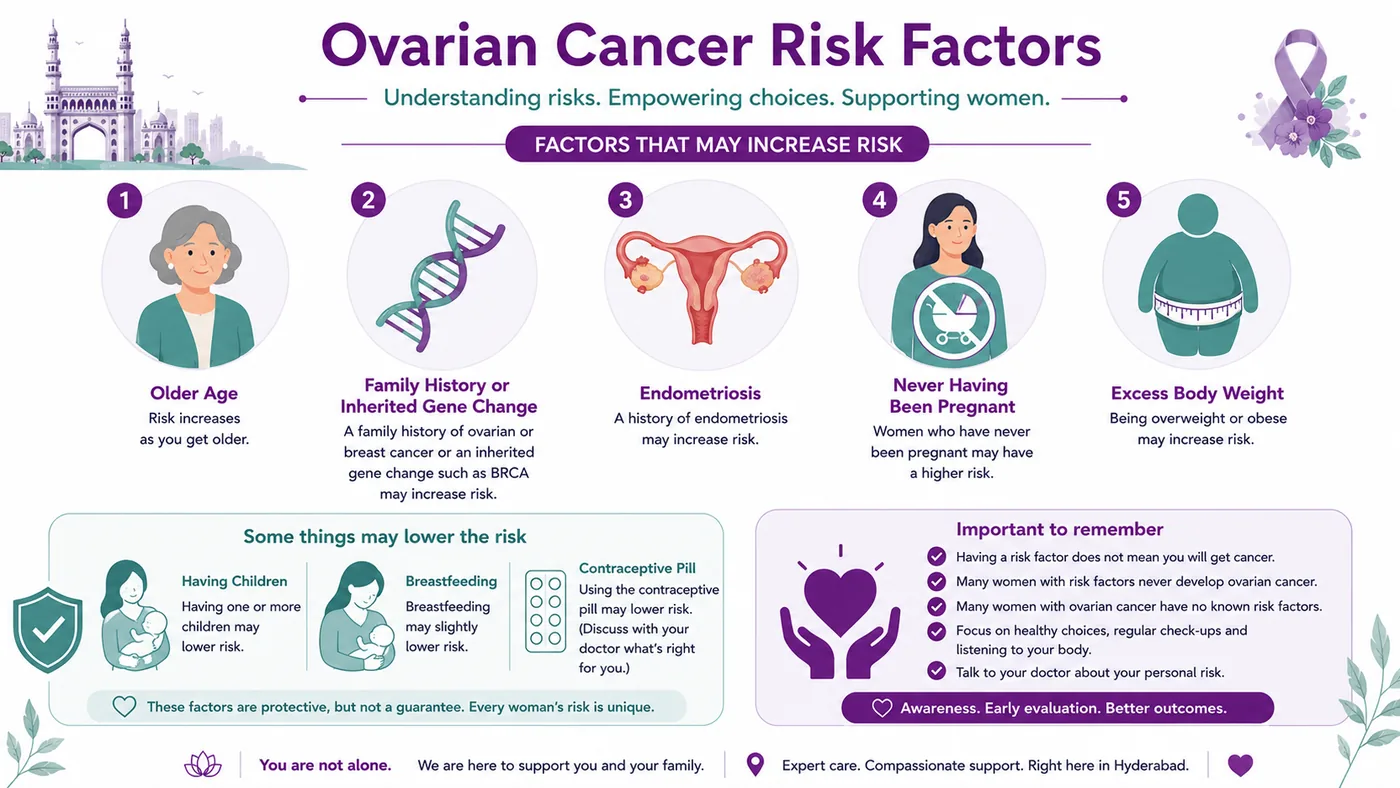
The biggest risk factors for ovarian cancer are getting older and an inherited gene change (like BRCA) or family history; endometriosis, never having been pregnant and a late menopause also play a part. Encouragingly, some things lower the risk — having children, breastfeeding, and the contraceptive pill. Having a risk factor doesn’t mean you’ll get ovarian cancer.
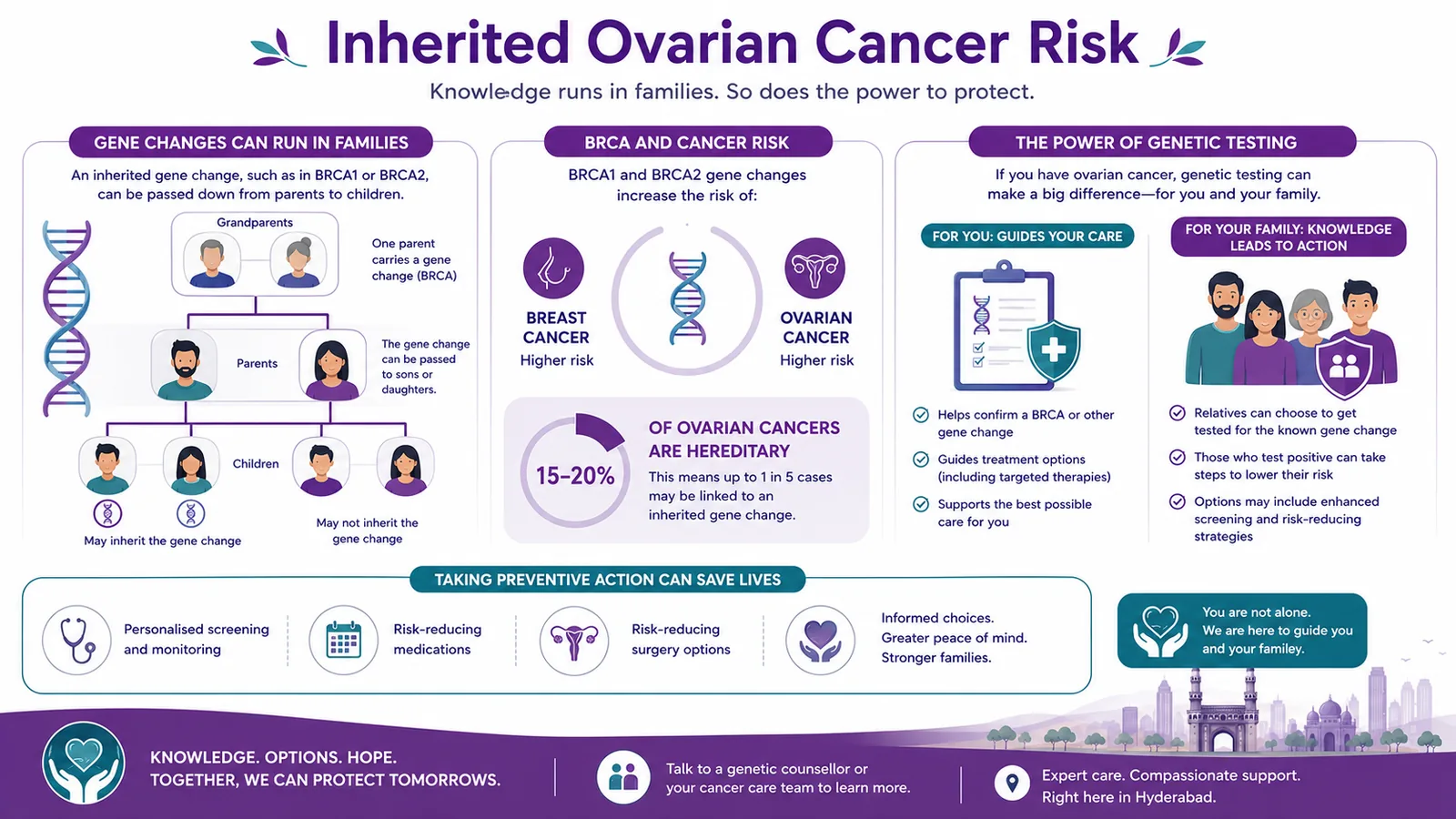
This is one of the most important things to know about ovarian cancer: a significant share — as many as 1 in 5 — is linked to an inherited gene change, most often BRCA1 or BRCA2 (the same genes behind much hereditary breast cancer). That’s why genetic testing is now recommended for everyone diagnosed with ovarian cancer — it can guide treatment (some maintenance therapies work especially well in BRCA-related cancer) and, just as importantly, lets your relatives find out their own risk and take preventive action.
Test everyone
Genetic testing is recommended for everyone with ovarian cancer, whatever the family history.
It guides treatment
A BRCA result can open up maintenance therapies that work especially well in BRCA-related cancer.
It protects your family
Relatives can learn their own risk and, if they carry it, take proven preventive steps.
Most ovarian cancers are “epithelial,” and the commonest and most aggressive of these is high-grade serous carcinoma. A separate group, germ cell tumours, mostly affect younger women and are usually highly treatable, even curable. Rarer stromal tumours make hormones and are often found early.
Understand the types
Simplified for understanding. Your exact type is confirmed by your team and guides your personalised plan.
Staging
The stages of ovarian cancer
Ovarian cancer is staged I to IV: from cancer confined to the ovaries or tubes (I), through spread within the pelvis (II) and to the abdomen or lymph nodes (III), to distant spread (IV). Many ovarian cancers are found at stage III — but, as the treatment section explains, even advanced ovarian cancer often responds very well.
Understand the stages
Simplified for understanding. Your exact stage and plan are confirmed by your team after tests and surgery.
Diagnosis
How ovarian cancer is diagnosed
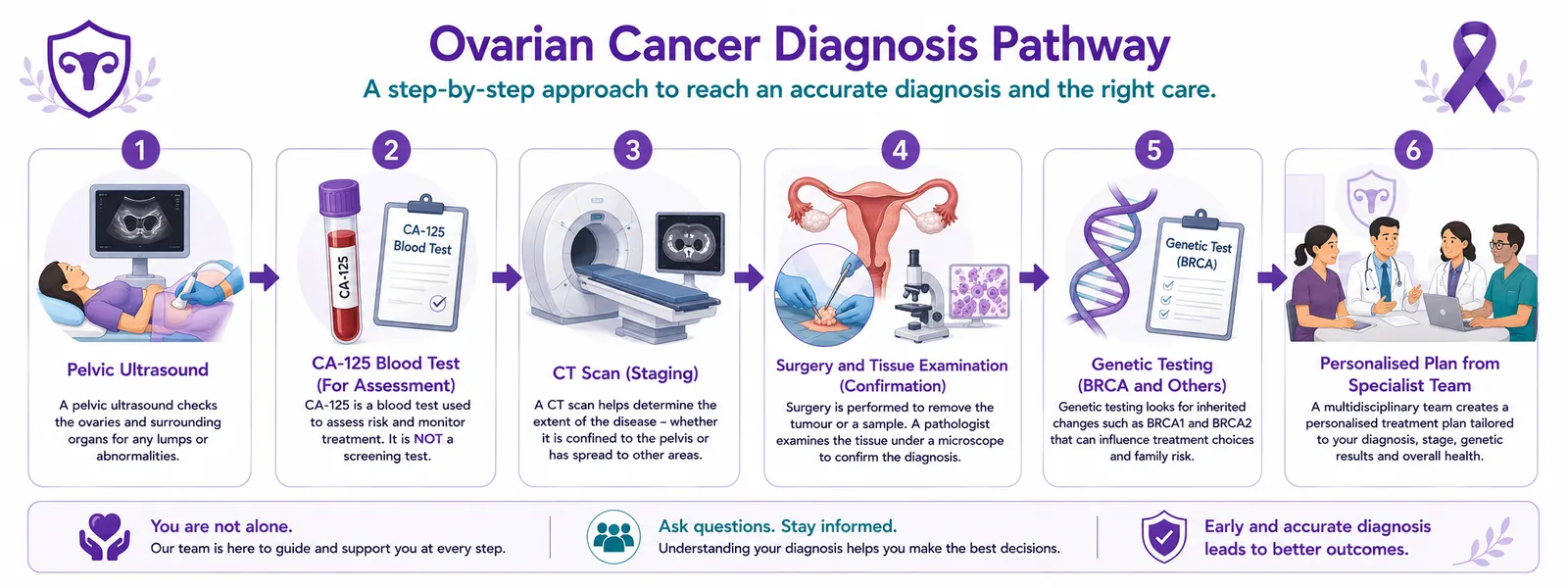
Ovarian cancer is assessed with a pelvic ultrasound and a CA-125 blood test, and a CT scan to see how far it has spread; the diagnosis is often confirmed at surgery, when tissue is examined. Importantly, everyone diagnosed is offered genetic testing. One honest point: CA-125 and ultrasound are used for assessment, not as a screening test for healthy women — there isn’t a reliable screening test for average-risk women.
From ultrasound and blood tests to surgery, tissue diagnosis and genetic testing.
Diagnostic services we offer — book any of these directly:
Pelvic ultrasound
A first-line scan that looks at the ovaries and pelvis for cysts or masses.
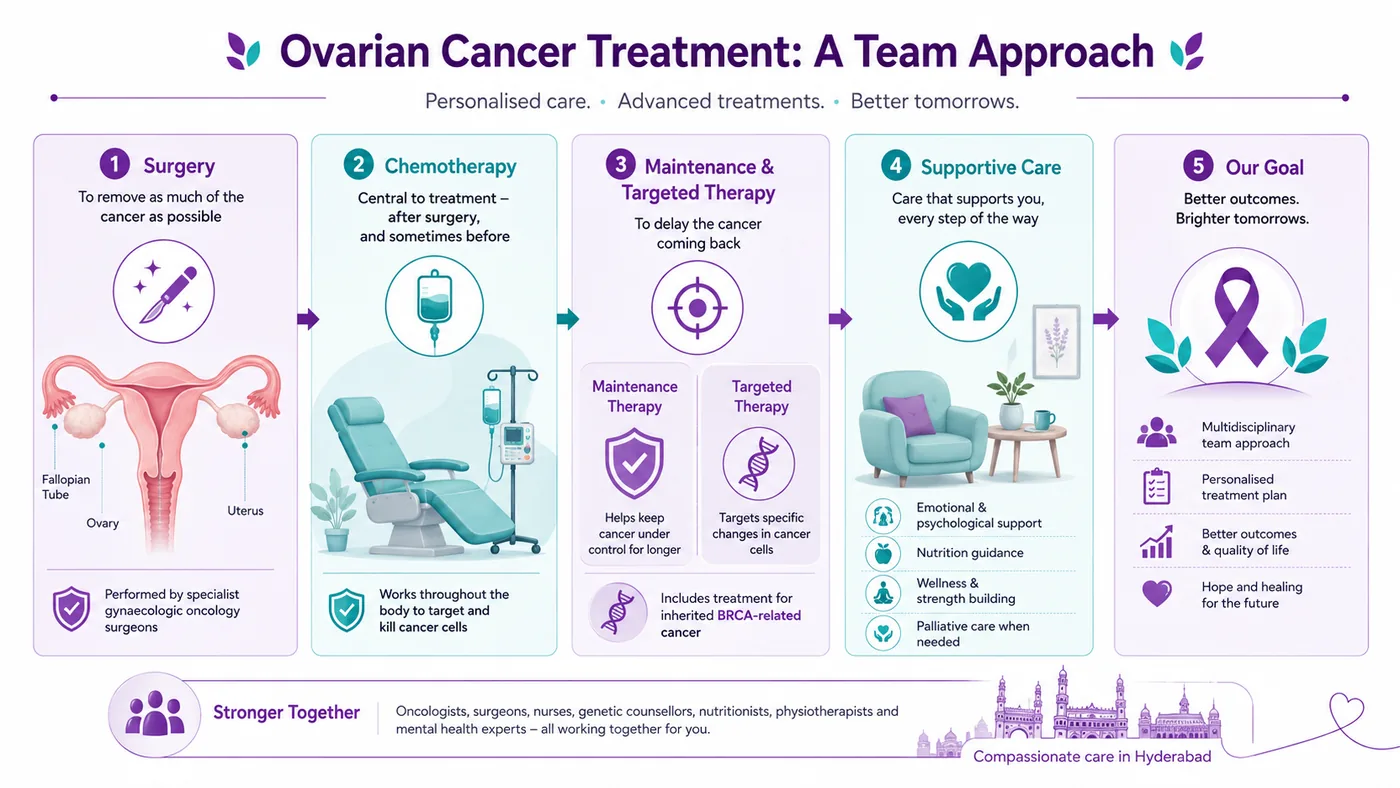
Ovarian cancer is treated by a multidisciplinary team, and the two mainstays are surgery and chemotherapy. Surgery aims to remove as much of the cancer as possible (“debulking”), and chemotherapy — to which ovarian cancer is unusually sensitive — is given afterwards, and sometimes first. For many women, maintenance or targeted therapy then follows, delaying the cancer’s return — and it works especially well in BRCA-related cancer. See our full guide to ovarian cancer treatment in Hyderabad.
A coordinated team. CION provides medical oncology (chemotherapy and maintenance therapy) in-house, and works with specialist gynaecologic-oncology surgeons for the surgery — so your whole pathway is planned and managed together. Radiation has a limited, mainly symptom-relieving role in ovarian cancer.
Treatments & care we coordinate — book a consult for any of these:
Debulking surgery (coordinated)
Removing as much of the cancer as possible — coordinated with specialist gynaecologic-oncology surgeons.
Here’s something important, especially if you’ve been told the cancer is advanced: ovarian cancer is one of the cancers that responds most strongly to chemotherapy. Most women — even with stage III disease — go into remission after surgery and chemotherapy. It can come back, but modern maintenance therapy (especially for BRCA-related cancer) is increasingly good at keeping it away for longer, and further treatment works when it’s needed. Advanced does not mean untreatable.
Unusually chemo-sensitive
Ovarian cancer responds to chemotherapy better than most cancers.
Remission is common
Most women reach remission after surgery and chemotherapy, even at stage III.
Maintenance helps it last
Modern maintenance therapy delays recurrence, especially in BRCA-related cancer.
Cost
Indicative cost of ovarian cancer treatment in Hyderabad
Cost varies widely with the stage and treatment — and surgery is delivered at specialist partner centres and may be billed there. It’s best given as an indicative range after assessment. Eligible treatment may be covered under Aarogyasri / PMJAY at empanelled centres.
Estimate an indicative range
Indicative range
—
Figures are indicative only and not a quotation — surgery may be delivered and billed at specialist partner centres, and maintenance therapy runs over many months. For an accurate estimate, request a callback.
Worrying symptoms, a pelvic scan finding, or a family history of ovarian or breast cancer shouldn’t wait. Book a free consultation and, if you already have a report, a free written second opinion.
Reviewed by a medical oncologist and gynae-oncology tumour board
Genetic counselling & BRCA testing for you and your family
Aarogyasri / PMJAY & insurance guidance
Support
Financial support & Aarogyasri
Cost should not delay care. Under Aarogyasri and PMJAY, eligible ovarian cancer treatment may be largely covered at empanelled centres. Our team helps check eligibility and guides you on insurance and EMI.
9 clinics in Hyderabad · 35+ across Telangana & AP
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the oncologists
Ovarian cancer is treated by a team, not one doctor.
Care is led by medical oncology, with radiation oncology and a coordinated gynaecologic-oncology surgical team — part of 17 senior specialists across CION.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Bloating or pelvic pain most days for weeks? Get it checked.
Early action means simpler treatment and better outcomes — and a family history of ovarian or breast cancer is worth discussing. Our oncologists see these cases every day.
The worries and myths we hear most about ovarian cancer, and the facts.
“Ovarian cancer has no symptoms — you can’t catch it early.”
Fact: It’s not silent — persistent bloating, fullness, pelvic pain and urinary urgency are real signs; knowing them helps catch it sooner.
“Bloating means I have ovarian cancer.”
Fact: Occasional bloating is very common and almost never cancer — it’s new, frequent bloating lasting most days for weeks that should be checked.
“A family history of breast cancer has nothing to do with ovarian cancer.”
Fact: The same genes (BRCA) drive both — a family history of either can mean inherited risk, which genetic testing can clarify.
“There’s a routine screening test I should be having.”
Fact: There’s no reliable screening for average-risk women — knowing the symptoms and your family history matters more.
“Advanced ovarian cancer can’t be treated.”
Fact: Ovarian cancer responds unusually well to chemotherapy; most women reach remission, and maintenance therapy helps keep it away.
“An ovarian cyst means cancer.”
Fact: Most cysts are benign and often resolve on their own, especially before menopause. A scan (and sometimes a blood test) helps tell them apart.
“A biopsy or surgery will make the cancer spread.”
Fact: Diagnosis and surgery are safe, standard steps done under controlled conditions. The real risk is delay, which lets a treatable cancer grow.
“Cancer is contagious — I could catch it from someone.”
Fact: Ovarian cancer is not infectious. You can’t catch it by living with, caring for or being close to someone who has it.
“If there’s no pain, it can’t be serious.”
Fact: Early ovarian cancer is often painless or only mildly uncomfortable. Persistent, frequent symptoms — not pain — are the signal to act on.
“Genetic testing will only frighten my family.”
Fact: Knowing about a BRCA change is empowering — relatives can choose testing, and those who carry it can take proven steps to lower their risk.
“Treatment is unaffordable — we can’t manage it.”
Fact: Under Aarogyasri and PMJAY, eligible treatment may be largely covered at empanelled centres. We help check eligibility, insurance and EMI.
“Chemotherapy always means being bedridden and losing all my hair.”
Fact: Side effects vary and are actively managed today. Many women continue much of daily life through treatment, with support at every step.
“A hysterectomy means my life as a woman is over.”
Fact: Surgery is about treating the cancer and living well afterwards. Menopause and wellbeing are actively supported, and many women return to full lives.
“Once ovarian cancer comes back, there’s no point treating it.”
Fact: Recurrent ovarian cancer is still very treatable — it stays sensitive to chemotherapy, and further treatment can control it and preserve quality of life.
“Home remedies alone can cure it.”
Fact: Relying on unproven remedies wastes the window when ovarian cancer is most treatable. Discuss anything complementary with your oncology team, not as a replacement.
“A second opinion will offend my doctor or waste time.”
Fact: A second opinion is normal and welcomed in cancer care — it confirms the plan and gives you confidence. At CION it’s free with a report.
“Only older women get ovarian cancer.”
Fact: Risk rises with age, but younger women get it too — germ cell tumours in particular affect younger women, and are usually highly treatable.
“If I ignore the symptoms, they’ll probably just go away.”
Fact: Symptoms that are new, frequent and last most days for weeks don’t need ignoring — they need checking. Most turn out harmless, and acting early matters.
Why CION
Why choose CION for ovarian cancer care
Chemotherapy & maintenance expertise
Platinum chemotherapy and modern maintenance/targeted therapy, including for BRCA-related cancer — led by medical oncology.
Genetic counselling & BRCA testing
Testing for you and your family, with counselling to make sense of the results.
Coordinated gynae-oncology surgery
Debulking surgery and hysterectomy via specialist gynaecologic-oncology surgeons — planned together.
Symptom awareness
Helping women recognise the real (if subtle) signs — because ovarian cancer isn’t truly silent.
Complete women’s-cancer care
Ovarian, cervical and endometrial cancer expertise, discussed by a gynae-oncology tumour board.
Close, NABH-accredited care
9 clinics across Hyderabad and 35+ across Telangana, within NABH-accredited facilities.
Real stories · real courage
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
Not exactly — it is better thought of as a "whispering" cancer. It does cause symptoms — persistent bloating, feeling full quickly, pelvic pain and urinary urgency — but they are subtle and easy to dismiss. Knowing them, and seeing a doctor when they are new, frequent and last most days for a few weeks, is the best way to catch it sooner.
What are the early warning signs of ovarian cancer?
The four symptoms that matter most are persistent bloating, feeling full quickly or difficulty eating, pelvic or lower-tummy pain, and needing to pass urine urgently or more often. Fatigue, a change in bowel habit and back pain can also occur. The pattern to act on is symptoms that are new, happen most days, and are frequent — especially if they last more than two to three weeks.
Is my bloating a sign of ovarian cancer?
Almost always, no — occasional bloating is extremely common and usually harmless. What matters is bloating (or feeling full quickly, pelvic pain, or urinary urgency) that is new, happens most days, and does not settle over two to three weeks. That deserves a check — not to alarm you, but because catching ovarian cancer sooner makes a real difference.
Is there a screening test for ovarian cancer?
Not a reliable one for women at average risk. CA-125 blood tests and ultrasound scans are not recommended as screening because they miss cancers and cause false alarms. The best protection is knowing the symptoms and knowing your family history, so that inherited (BRCA) risk can be identified and managed. Women at high inherited risk should discuss a personalised plan with a specialist.
My mother or sister had breast or ovarian cancer — should I get a BRCA test?
It is worth discussing with a doctor. A family history of ovarian or breast cancer — especially at a young age or in several relatives — can point to an inherited gene change like BRCA1 or BRCA2. Genetic counselling and a test can clarify your risk, and if you carry it, there are proven ways to lower your chances. Everyone diagnosed with ovarian cancer is also offered genetic testing.
What is BRCA, and how is it linked to ovarian cancer?
BRCA1 and BRCA2 are genes that normally help protect against cancer. An inherited change (mutation) in one of them raises the risk of both ovarian and breast cancer — which is why a family history of either matters. As many as 1 in 5 ovarian cancers are linked to an inherited gene change. Knowing your BRCA status can guide treatment and lets relatives take preventive action.
I have an ovarian cyst — is it cancer?
Most likely not. The great majority of ovarian cysts, especially before menopause, are benign and often disappear on their own. A scan, and sometimes a blood test, help tell reassuring cysts from ones that need follow-up. Your doctor will advise whether anything more is needed — a cyst is not the same as cancer.
What causes ovarian cancer and who is at higher risk?
Most ovarian cancers do not have a single identifiable cause. The strongest risk factors are increasing age and an inherited gene change (like BRCA) or a family history of ovarian or breast cancer. Endometriosis, never having been pregnant, and a late menopause also play a part. Some things lower risk, including having children, breastfeeding and the contraceptive pill. Having a risk factor does not mean you will get ovarian cancer.
What are the types of ovarian cancer?
Most ovarian cancers are "epithelial," and the commonest and most aggressive of these is high-grade serous carcinoma, which is often linked to BRCA. A separate group, germ cell tumours, mostly affect younger women and are usually highly treatable, even curable. Rarer sex cord-stromal tumours arise from the ovary’s hormone-producing tissue and are often found early.
How is ovarian cancer diagnosed?
Assessment usually starts with a pelvic ultrasound and a CA-125 blood test, followed by a CT scan to see how far the cancer has spread. The diagnosis is often confirmed at surgery, when tissue is examined under a microscope. Everyone diagnosed is offered genetic (BRCA) testing. Importantly, CA-125 and ultrasound are used for assessment, not as a screening test for healthy women.
What is CA-125?
CA-125 is a protein that can be raised in the blood in ovarian cancer. It is useful for assessing a suspicious finding and for monitoring treatment, but it is not a screening test — it can be normal in some cancers and raised by many harmless conditions such as endometriosis, fibroids or even menstruation. Your doctor interprets it alongside your scans and symptoms.
What are the stages of ovarian cancer?
Ovarian cancer is staged I to IV. Stage I is confined to one or both ovaries or fallopian tubes; stage II has spread within the pelvis; stage III has spread to the abdominal lining or lymph nodes; and stage IV has spread to distant organs. Many ovarian cancers are found at stage III — and, because the cancer responds so well to chemotherapy, even advanced disease is often very treatable.
Is ovarian cancer curable?
It can be, especially when found early — and even advanced ovarian cancer is very treatable, because it responds unusually well to chemotherapy. Most women reach remission after surgery and chemotherapy; it can return, but modern maintenance therapy (especially for BRCA-related cancer) increasingly keeps it away for longer. Germ cell tumours in younger women are often curable even when advanced.
Can advanced (stage III or IV) ovarian cancer be treated?
Yes. Ovarian cancer is one of the cancers that responds most strongly to chemotherapy, so even advanced disease is often very treatable. Most women — even at stage III — reach remission after surgery and chemotherapy. If it comes back, it usually stays sensitive to further treatment, and maintenance therapy helps keep it away for longer. Advanced does not mean untreatable.
How is ovarian cancer treated?
The two mainstays are surgery and chemotherapy, planned by a multidisciplinary team. Surgery ("debulking") aims to remove as much of the cancer as possible and is coordinated with specialist gynaecologic-oncology surgeons; chemotherapy is given afterwards, and sometimes before. Many women then have maintenance or targeted therapy to delay the cancer’s return — this works especially well in BRCA-related cancer. Radiation has a limited, mainly symptom-relieving role.
What is debulking (cytoreductive) surgery?
Debulking, or cytoreductive surgery, aims to remove as much of the visible cancer as possible — often including the ovaries, fallopian tubes and uterus. Removing more of the cancer generally improves how well chemotherapy works. At CION this surgery is coordinated with specialist gynaecologic-oncology surgeons, while medical oncology (chemotherapy and maintenance therapy) is provided in-house, so the whole pathway is planned together.
What is maintenance therapy?
Maintenance therapy is treatment given after surgery and chemotherapy to delay the cancer coming back. Modern maintenance and targeted therapies have improved how long remission lasts, and some of them work especially well in cancers linked to a BRCA change — another reason genetic testing matters. Your oncologist advises whether maintenance therapy is right for your situation.
How much does ovarian cancer treatment cost in Hyderabad?
Cost varies widely with the stage and treatment plan, and surgery may be delivered and billed at specialist partner centres, so it is best given as an indicative range after assessment. Eligible treatment may be covered under Aarogyasri or PMJAY at empanelled centres, and our team helps with insurance and EMI. Use the cost estimator on this page for an indicative figure, then request a callback for an accurate estimate.
Can ovarian cancer be prevented or the risk reduced?
There is no guaranteed way to prevent ovarian cancer, but some factors lower the risk, including having children, breastfeeding and the contraceptive pill. For women with a known BRCA change or strong family history, options such as enhanced monitoring and risk-reducing surgery can substantially lower risk — which is why genetic counselling is so valuable. Knowing your family history is the most important first step.
Will treatment cause menopause or affect fertility?
It can, because surgery may remove the ovaries. For younger women, fertility-sparing options are sometimes possible, particularly with germ cell tumours — this is discussed before treatment where appropriate. Where surgery brings on menopause, symptoms and long-term wellbeing are actively supported. Ask your team about fertility and menopause early, so your plan takes your priorities into account.
Explore
Explore ovarian & women’s cancer care
Our guide to ovarian cancer — treatment, doctors, the BRCA link, tests and support — plus the wider women’s-cancer cluster. Tap any topic to read more.
Worrying symptoms, or a family history? Talk to a specialist.
Persistent bloating, feeling full quickly or pelvic pain that lasts most days deserves a check — and if ovarian or breast cancer runs in your family, genetic counselling can clarify your risk. Book a consultation or second opinion at any of our 9 Hyderabad clinics, part of 35+ centres across Telangana & Andhra Pradesh.
Medical disclaimer: This page is for general information and awareness and does not replace professional medical advice, diagnosis or treatment. Severe abdominal pain or swelling, or persistent symptoms, need timely medical attention. Always consult a qualified oncologist or gynaecologic oncologist. Costs shown are indicative only and not a quotation. Content is periodically reviewed by CION’s medical team.