
Hyderabad's Dedicated Kidney Cancer Team
Kidney Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Kidney cancer — most commonly renal cell carcinoma (RCC) — is one of the few cancers where early detection leads to cure in the vast majority of cases. Many tumours are caught incidentally on imaging, giving patients a treatment advantage when they act with the right specialist team. At CION Cancer Clinics, our surgical, medical and radiation oncology team delivers the full spectrum of kidney cancer care — from nephron-sparing surgery and laparoscopic nephrectomy to the latest NCCN-approved combination immunotherapy for advanced disease.
- Nephron-Sparing First — partial nephrectomy preferred wherever oncologically safe, preserving long-term kidney function
- NCCN Immunotherapy Combinations — Nivolumab + Ipilimumab and Pembrolizumab + Axitinib for advanced RCC
- Tumour Board for Every Patient — surgical, medical & radiation oncology decisions together, not one doctor's call
- 7 Locations, NABH Accredited — Aarogyasri empanelled, EMI available, 1,000+ kidney cancer cases treated yearly
17+
Cancer Specialists
on Panel
on Panel
96.9%
Breast Cancer
Survival Rate*
Survival Rate*
15,000+
Patients
Treated
Treated
4.8★
Google Rating
(800+ reviews)
(800+ reviews)
Kidney Cancer in Hyderabad — What You Need to Know
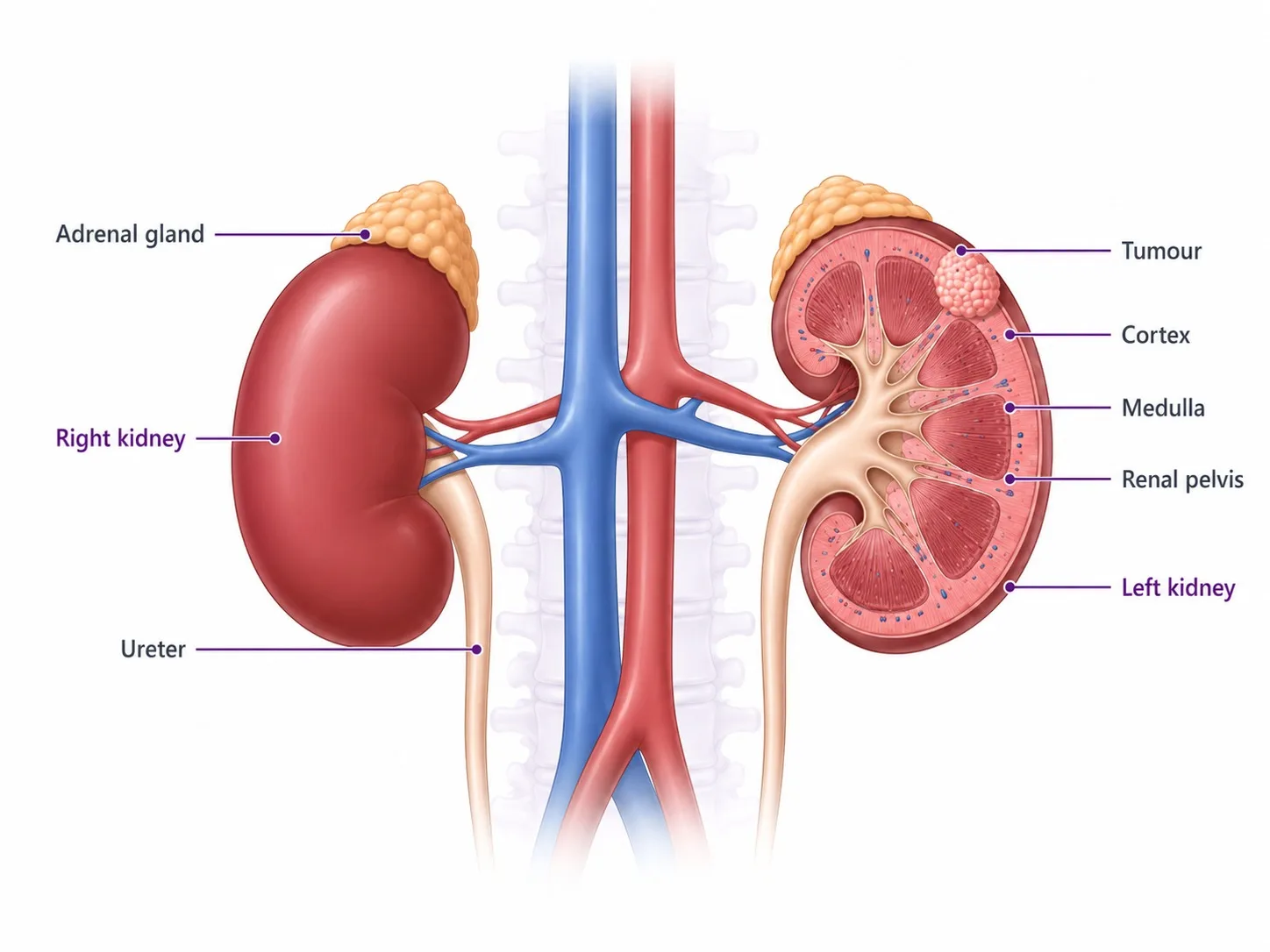
Kidney cancer develops when cells in the kidney begin to grow uncontrollably, forming a tumour. Renal cell carcinoma (RCC) is the most common type, accounting for approximately 85% of all kidney cancers in adults. The remaining 15% include urothelial carcinoma of the renal pelvis, rare sarcomas, and in children, Wilms tumour (nephroblastoma).
Hyderabad's rising rates of hypertension, obesity, and Type 2 diabetes — all recognised risk factors for RCC — are contributing to increasing kidney cancer incidence across the city. The encouraging reality is that kidney cancer detected at Stage I or II has five-year survival rates exceeding 90%, and many patients are cured with surgery alone.
The choice of treatment centre matters considerably — particularly for decisions around nephron-sparing surgery, access to current immunotherapy combinations, and coordination of robotic surgical referral when minimally invasive techniques beyond standard laparoscopy are required.
Did You Know? Approximately 25–30% of kidney cancers are discovered incidentally — detected during imaging performed for an unrelated condition before any symptoms appear. These incidental tumours are typically at an early, highly curable stage. If you have not had a routine abdominal ultrasound and are in a high-risk group, speak to your oncologist.
Types of Kidney Cancer We Treat
Not every kidney cancer behaves the same way. CION's tumour board evaluates each patient's diagnosis at the cellular and molecular level so treatment is matched precisely to the subtype.
Renal Cell Carcinoma (RCC)
The dominant form of kidney cancer in adults. RCC develops in the proximal renal tubules — the small filtering tubes of the kidney — and is further classified by cell type:
- Clear Cell RCC — ~80% of all RCCs; driven by VHL mutations; responds well to VEGF-targeted therapy and immune checkpoint inhibitors
- Papillary RCC — ~15% of RCCs; Type 1 generally indolent, Type 2 more aggressive
- Chromophobe RCC — ~5%; generally low-grade with a favourable prognosis
- Sarcomatoid / Rhabdoid Differentiation — a high-grade feature in any subtype; treated with combination immunotherapy
- Collecting Duct & Medullary RCC — rare, aggressive subtypes requiring specialist management
Urothelial Carcinoma of the Renal Pelvis
Develops in the transitional cells lining the renal pelvis — the funnel-shaped structure where urine collects before passing to the ureter. Treated similarly to bladder cancer with nephroureterectomy and chemotherapy, with long-term surveillance for bladder recurrence.
Wilms Tumour (Nephroblastoma)
A paediatric kidney cancer occurring predominantly in children under 5 years. Highly chemosensitive and curable in the majority of cases with a combination of neoadjuvant chemotherapy, surgery, and radiation therapy where required. Managed through CION's paediatric oncology pathway.
Hereditary Kidney Cancer Syndromes
Approximately 5–8% of kidney cancers are hereditary:
- Von Hippel-Lindau (VHL) Disease — clear cell RCC, often bilateral and multifocal
- Birt-Hogg-Dubé (BHD) Syndrome — chromophobe and clear cell RCC; skin lesions; pulmonary cysts
- Hereditary Papillary RCC — MET mutation; multiple bilateral papillary Type 1 tumours
- HLRCC — FH mutation; aggressive papillary Type 2 RCC
CION offers genetic counselling for patients with early-onset, bilateral, or familial kidney cancer.
Risk Factors for Kidney Cancer
Understanding your personal risk is critical — particularly with Hyderabad's rising rates of hypertension, obesity, and Type 2 diabetes, all of which are linked to RCC.
- Smoking — doubles the risk of RCC; one of the most modifiable risk factors
- Obesity and overweight — rising rapidly in urban Hyderabad; independently associated with increased RCC risk
- Uncontrolled hypertension — both the condition and certain antihypertensive medications are associated with elevated risk
- Long-term dialysis — patients on haemodialysis develop acquired cystic kidney disease, which significantly raises RCC risk
- Type 2 diabetes — associated with increased RCC incidence
- Hereditary conditions — VHL disease, Birt-Hogg-Dubé syndrome, hereditary papillary RCC
- Family history of kidney cancer — first-degree relatives carry a 2–4 times higher risk
- Chronic occupational exposure — trichloroethylene, cadmium, asbestos
If you have any of these risk factors, an abdominal ultrasound during routine check-ups is a low-cost way to catch a tumour early — before symptoms appear.
Symptoms of Kidney Cancer
Kidney cancer is often called a 'silent' tumour — the classic triad of symptoms (blood in urine, flank pain, and palpable abdominal mass) occurs together in fewer than 10% of patients, and many early-stage tumours produce no symptoms at all. Signs to be aware of include:
- Haematuria — blood in the urine (visible or detected on urinalysis); the most common presenting symptom
- Persistent pain or aching in the flank, side, or lower back — not related to injury
- A palpable lump or mass in the side or abdomen
- Unexplained weight loss
- Fatigue and persistent anaemia
- Persistent fever without an identifiable infection
- High blood pressure that is difficult to control
- Swelling in the legs or ankles (from venous obstruction)
If you notice blood in the urine — even once — consult a specialist immediately. Haematuria is never normal and warrants prompt investigation — you can hear one patient describe how spotting blood in his urine led to his kidney cancer diagnosis. Speak to a CION kidney cancer oncologist if you have symptoms or known risk factors.
Why Patients Choose CION for Kidney Cancer Treatment in Hyderabad
Sixteen reasons our patients pick CION — nephron-sparing surgery as default, active surveillance, genetic counselling, and full integrative support.
1,000+ kidney cancer cases
7 locations across Hyderabad
5-Star NABH Accredited
NCCN Protocol Adherence
Nephron-sparing surgery as default
Laparoscopic nephrectomy
Robotic-assisted nephrectomy referral
Active surveillance programme
Genetic counselling
Multidisciplinary tumour board review
Full integrative support
Dedicated Second Opinion service
Aarogyasri empanelled
EMI facility
4.8 / 5 Google rating
35+ centres across Telangana & AP
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.






Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centre
Beyond Hyderabad
35+ centres across Telangana & Andhra Pradesh
Travelling for treatment? We may have a centre right where you are.
Telangana
Andhra Pradesh
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.

Medical Oncologist

Medical Oncologist
Dr. C. Raghavendra Reddy
MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

Medical Oncologist
Dr. Bharati Devi Gorantla
MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

Medical Oncologist
Dr. Owais Mohammed
MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)

Medical Oncologist

Medical Oncologist

Surgical Oncologist
Dr. Muralidhar Muddusetty
MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)

Surgical Oncologist

Surgical Oncologist

Surgical Oncologist
Dr. Vinay Mamidala
MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)

Surgical Oncologist

Radiation Oncologist

Radiation Oncologist

Radiation Oncologist

Hematologist

Interventional Radiologist
Dr. Mohammed Imran

Surgical Oncologist
Dr. Vajja Sandeep Kumar
MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Surgical Oncologist
Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationBook an appointment with our specialist
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Get a Second Opinion Before Nephrectomy
Our multidisciplinary tumour board reviews your imaging and pathology — especially important when kidney-sparing surgery may be an option you have not yet been offered.
Kidney Cancer Diagnosis at CION
Kidney cancer diagnosis is primarily imaging-driven. Unlike most other cancers, biopsy is not routinely required — the imaging characteristics of kidney tumours on CT or MRI are often sufficient for diagnosis. CION's diagnostic pathway is streamlined to reach a treatment decision efficiently.
Imaging
- Ultrasound — first-line investigation for haematuria or flank pain; identifies solid vs cystic lesions
- CT Scan (with contrast, multiphasic) — the gold standard for kidney cancer diagnosis and staging; characterises enhancement patterns that distinguish RCC from benign lesions
- MRI — preferred for patients with contrast allergy, renal impairment, or indeterminate CT findings; most accurate for assessing venous thrombus extension
- Chest CT — standard staging investigation to assess for pulmonary metastases
- Bone scan / Brain MRI — for patients with symptoms or elevated alkaline phosphatase suggesting bone or brain spread
Blood and Urine Tests
- Full blood count, renal function, LFTs, serum calcium — baseline assessment and paraneoplastic workup
- Urine cytology — for urothelial carcinoma of the renal pelvis when transitional cell involvement is suspected
Biopsy
Renal mass biopsy is performed selectively at CION — not routinely. It is indicated when imaging is indeterminate, when a small renal mass is being considered for active surveillance, or when metastatic disease needs histological confirmation before systemic therapy. Image-guided core needle biopsy is used where indicated.
Kidney Cancer Staging — TNM and Clinical Stage
Kidney cancer is staged using the TNM (Tumour, Node, Metastasis) system. Stage directly determines the treatment approach. The table below maps clinical stages to standard treatment options as per current NCCN guidelines.
| Stage | Tumour Status | Lymph Nodes / Metastasis | Primary Treatment |
|---|---|---|---|
| Stage I | Tumour ≤7cm, confined to kidney (T1) | No nodes, no metastasis | Partial or radical nephrectomy; active surveillance for T1a <4cm in select patients |
| Stage II | Tumour >7cm, confined to kidney (T2) | No nodes, no metastasis | Radical nephrectomy; partial nephrectomy where technically feasible |
| Stage III | Extends into major veins or perinephric tissue (T3); or regional lymph nodes (N1) | Regional nodes only | Radical nephrectomy + lymph node dissection; adjuvant pembrolizumab for high-risk resected RCC |
| Stage IV | Extends beyond Gerota's fascia (T4) or distant metastasis (M1) | Any N, M1 | Cytoreductive nephrectomy (select cases) + systemic therapy; or systemic therapy alone |
Treatment decisions are always individualised by CION's multidisciplinary tumour board based on performance status, renal function, risk stratification, and patient preference.
Kidney Cancer Treatment at CION Cancer Clinics
CION follows NCCN protocol-driven treatment planning for all kidney cancer subtypes. Every case is reviewed by a multidisciplinary tumour board before treatment begins.
Surgical Oncology — Nephron-Sparing First
Surgery is the cornerstone of curative kidney cancer treatment. CION prioritises nephron-sparing approaches wherever oncologically appropriate — preserving kidney function and reducing the long-term risk of chronic kidney disease.
- Partial Nephrectomy — preferred for T1 tumours; gold standard for T1a (≤4cm)
- Radical Nephrectomy — for larger or centrally-located tumours, or with venous thrombus
- Laparoscopic Nephrectomy — minimally invasive option for eligible patients
- Cytoreductive Nephrectomy — selected Stage IV cases before systemic therapy
Robotic-Assisted Nephrectomy — Referral & Coordination
Robotic-assisted surgery offers enhanced precision and three-dimensional visualisation for complex partial nephrectomies — particularly for hilar tumours or those requiring intricate reconstruction. CION does not perform robotic surgery in-house. Patients who are candidates are referred to accredited robotic centres, while CION coordinates the complete journey — pre-surgical workup, referral, and post-operative oncology follow-up.
Active Surveillance for Small Renal Masses
Not every kidney tumour requires immediate surgery. For T1a tumours (under 4cm) — particularly elderly patients, those with significant comorbidities, or those with a single kidney — active surveillance is a recognised NCCN management option. CT or MRI every 3–6 months monitors growth; intervention is triggered only by meaningful progression. CION is one of the few oncology networks in Hyderabad to formally offer this pathway.
Ablation — RFA & Cryoablation
Radiofrequency Ablation (RFA) uses heat generated by electrical current to destroy small kidney tumours (T1a, <4cm) in patients unsuitable for surgery. Cryoablation delivers extreme cold via a probe to freeze and destroy tumour tissue. Both are image-guided, minimally invasive, and effective for small peripheral renal masses.
Radiation Therapy
The kidney is a relatively radiation-sensitive organ and conventional radiation has a limited role in primary RCC. CION uses advanced techniques in specific situations:
- SBRT — high-dose, focused radiation for small localised RCC unsuitable for surgery or ablation, and for oligometastatic disease
- Palliative radiation — for symptomatic bone or brain metastases, or local compression causing pain
Targeted Therapy & Systemic Options
For advanced or metastatic RCC, CION delivers all current NCCN preferred regimens — including combination immunotherapy (detailed in the next section), targeted oral TKIs (sunitinib, pazopanib, cabozantinib), and mTOR inhibitors (everolimus) for second-line and beyond. Adjuvant pembrolizumab is the recommended option following resection of high-risk Stage II or Stage III RCC per the Keynote-564 trial.
Advanced Kidney Cancer Treatment — Current NCCN Immunotherapy Combinations
The treatment of advanced and metastatic RCC has been transformed by combination immunotherapy. Single-agent sunitinib — once the standard of care — has now been largely replaced by combination regimens demonstrating superior survival. CION delivers current NCCN preferred protocols.
Nivolumab + Ipilimumab
NCCN Preferred · Intermediate/Poor Risk
The combination of nivolumab (PD-1 inhibitor) and ipilimumab (CTLA-4 inhibitor) is an NCCN preferred first-line regimen for intermediate and poor-risk advanced RCC. The CheckMate-214 trial demonstrated significantly improved overall survival and complete response rates compared to sunitinib — with durable responses persisting after treatment completion. CION administers this regimen with regular immune-related adverse event monitoring throughout treatment.
Pembrolizumab + Axitinib
NCCN Preferred · All Risk Groups
The combination of pembrolizumab (PD-1 inhibitor) and axitinib (VEGFR tyrosine kinase inhibitor) is an NCCN preferred first-line regimen for advanced RCC across all risk groups. The Keynote-426 trial demonstrated superior overall survival and progression-free survival versus sunitinib across all IMDC risk groups. This combination provides both immune activation and anti-angiogenic tumour suppression simultaneously.
Other NCCN Preferred Combinations
Additional First-Line
- Nivolumab + Cabozantinib (CheckMate-9ER) — PD-1 + multi-TKI; preferred for all risk groups
- Pembrolizumab + Lenvatinib (CLEAR trial) — highest progression-free survival in Phase 3 data
- Avelumab + Axitinib — preferred option for favourable-risk patients
- Sunitinib or Pazopanib — TKI monotherapy alternative when combination immunotherapy is contraindicated
Subsequent Therapy & Adjuvant Pembrolizumab
Second-Line & Adjuvant
- Nivolumab monotherapy after TKI progression
- Cabozantinib — multi-target TKI active after prior VEGF/mTOR therapy
- Everolimus / Temsirolimus — mTOR inhibitors after TKI progression
- Lenvatinib + Everolimus for first-line progressors
- Adjuvant Pembrolizumab — for high-risk resected Stage II/III RCC per the Keynote-564 trial
Did You Know? The Keynote-426 trial demonstrated that pembrolizumab + axitinib improved median overall survival to 45.7 months versus 40.1 months with sunitinib across all risk groups in advanced RCC — establishing combination immunotherapy as the new standard of care for kidney cancer.
Multidisciplinary Tumour Board — Every Case Reviewed by a Team
Kidney cancer management requires close coordination between surgical oncology, medical oncology, radiation oncology, and where appropriate, genetic counselling. At CION, every kidney cancer case is reviewed by a multidisciplinary tumour board ensuring:
- The correct surgical approach — partial vs radical nephrectomy vs active surveillance vs ablation
- Accurate IMDC risk stratification for advanced disease (to guide systemic therapy selection)
- Adjuvant pembrolizumab discussion for high-risk resected Stage II/III cases
- Cytoreductive nephrectomy evaluation for Stage IV patients before systemic therapy
- Genetic counselling referral for hereditary RCC patterns (early onset, bilateral, familial)
- Alignment with current NCCN evidence-based guidelines
- Digital coordination across all 7 Hyderabad locations
Kidney Cancer Treatment Cost in Hyderabad
Treatment costs vary based on cancer stage, surgical approach, and whether systemic therapy is required. The ranges below are indicative — CION provides a personalised cost estimate after your initial oncology consultation.
| Treatment | Approx. Cost (INR) | Notes |
|---|---|---|
| Partial Nephrectomy (Laparoscopic) | ₹2,00,000 – ₹4,50,000 | Preferred for T1 tumours; shorter hospital stay |
| Radical Nephrectomy (Laparoscopic) | ₹2,50,000 – ₹5,00,000 | Varies by extent of lymph node dissection |
| Radical Nephrectomy (Open) | ₹2,00,000 – ₹4,00,000 | For complex or large tumours |
| Ablation (RFA / Cryoablation) | ₹75,000 – ₹2,00,000 | Day-care procedure for small tumours |
| Targeted Therapy (per month) | ₹25,000 – ₹1,20,000 | Sunitinib / pazopanib oral; long-term maintenance |
| Combination Immunotherapy (per cycle) | ₹1,50,000 – ₹3,50,000+ | Nivolumab + ipilimumab / pembrolizumab + axitinib |
| Radiation Therapy (SBRT) | ₹1,50,000 – ₹3,00,000 | Per treatment course for oligometastatic disease |
| Full Multi-modal Treatment | ₹2,00,000 – ₹8,00,000+ | Depending on stage and treatment sequence |
Financial Support Options
- Aarogyasri Scheme — cashless treatment coverage for eligible Telangana residents (White Ration Card holders)
- EMI Facility — flexible instalment-based payment options available for all patients
- Private Health Insurance — CION works with all major TPAs for cashless hospitalisation
Real outcomes, real patients
You deserve a team that walks this journey with you
1,000+ cancer cases treated yearly. Decisions made by a tumour board, not a single doctor. Costs explained upfront, every time.
Real Stories. Real Voices.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
























Read all 800+ reviews on Google
Start Your Story. Book Free Consultation.Frequently Asked Questions
Common questions about kidney cancer treatment in Hyderabad — answered by CION's oncology team.
What is the best treatment for kidney cancer?
The best treatment depends on the stage and subtype of kidney cancer. For early-stage (Stage I and II) RCC, surgery — either partial or radical nephrectomy — is the standard curative approach, with partial nephrectomy preferred to preserve kidney function. For advanced or metastatic RCC, current NCCN preferred first-line treatments are combination immunotherapy regimens — nivolumab + ipilimumab or pembrolizumab + axitinib — which have demonstrated superior survival compared to earlier targeted therapy monotherapy. CION's multidisciplinary tumour board selects the most appropriate protocol for every individual patient.
What is the cost of kidney cancer treatment in Hyderabad?
Kidney cancer treatment costs in Hyderabad typically range from approximately ₹2,00,000 for laparoscopic partial nephrectomy to ₹8,00,000 or more for multi-modal treatment involving surgery and systemic immunotherapy. Monthly targeted therapy costs range from ₹25,000 to ₹1,20,000 depending on the drug. Combination immunotherapy cycles range from ₹1,50,000 to ₹3,50,000+ per cycle. CION provides a personalised estimate after your oncology consultation. Aarogyasri and EMI payment options are available.
Is kidney cancer curable in early stages?
Yes — kidney cancer has among the best early-stage prognosis of all solid tumours. Stage I RCC (tumour confined to the kidney, ≤7cm) has a five-year survival rate exceeding 90% following surgical resection. Stage II (tumour >7cm, still confined to the kidney) has a five-year survival of approximately 75%. Even Stage III disease has meaningful cure rates with surgery followed by adjuvant therapy where indicated. Early detection — whether through symptoms or incidental imaging — is the most important factor in achieving cure.
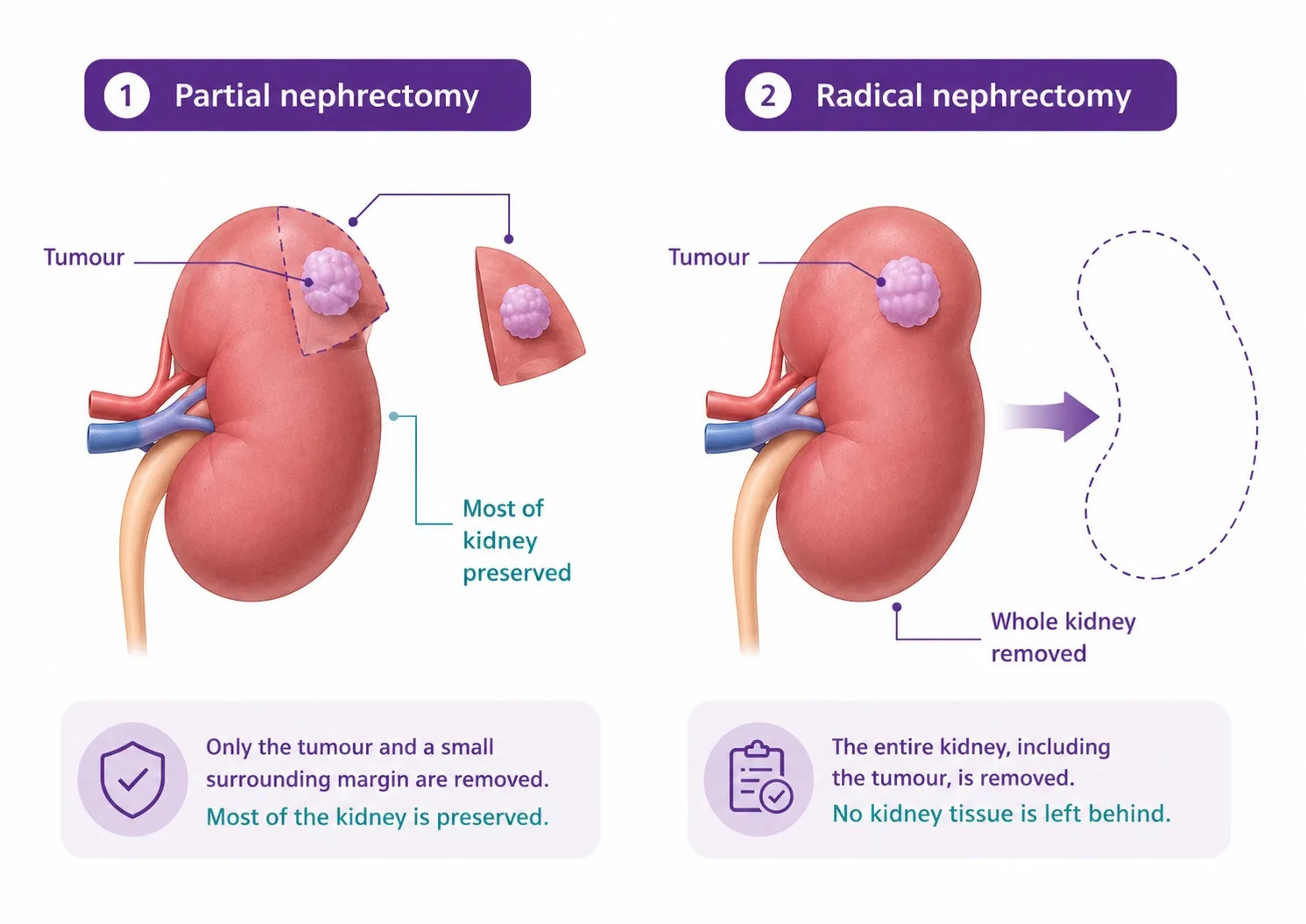
What is the difference between partial and radical nephrectomy?
Partial nephrectomy (nephron-sparing surgery) removes only the tumour and a margin of surrounding healthy kidney tissue, preserving the remainder of the kidney and its function. It is the preferred approach for T1 tumours (up to 7cm) and strongly preferred for T1a tumours (up to 4cm). Radical nephrectomy removes the entire affected kidney along with surrounding fat and, where indicated, regional lymph nodes. It is used for larger, centrally located, or more complex tumours where partial nephrectomy is not technically feasible. Both can be performed laparoscopically at CION for eligible patients.
What are the early signs of kidney cancer?
The most important early sign is blood in the urine (haematuria) — even a single episode warrants urgent specialist investigation. Other signs include persistent flank or lower back pain not related to injury, a palpable lump in the side or abdomen, unexplained weight loss, persistent fatigue, anaemia, or a fever without an identifiable infection. Importantly, many early kidney cancers produce no symptoms and are discovered incidentally during imaging for other conditions — reinforcing the value of routine health screening in high-risk individuals.
Can kidney cancer be treated without removing the kidney?
Yes, in several situations. Active surveillance is an NCCN-recognised option for very small tumours (T1a, under 4cm) in elderly patients or those with significant comorbidities, where the growth rate is monitored and intervention triggered only by meaningful progression. Ablation techniques — radiofrequency ablation (RFA) and cryoablation — destroy small tumours using heat or cold without surgical removal, and are suitable for patients not fit for surgery. Radiation therapy (SBRT) is also an option for selected inoperable cases. CION's tumour board evaluates every patient for nephron-sparing and non-surgical options before recommending nephrectomy.
What is the survival rate for kidney cancer in India?
Survival rates are strongly stage-dependent. Stage I RCC: five-year survival exceeds 90%. Stage II: approximately 75%. Stage III: 50–70% with surgery and adjuvant therapy. Stage IV (metastatic): historically poor, but modern combination immunotherapy (pembrolizumab + axitinib, nivolumab + ipilimumab) has significantly improved outcomes, with median overall survival now exceeding 40 months in clinical trial populations. Access to current NCCN-approved systemic therapies at a specialist oncology centre is the key determinant of outcomes in advanced disease.
What are the stages of kidney cancer?
Kidney cancer is staged using the TNM system. Stage I: tumour ≤7cm confined to the kidney. Stage II: tumour >7cm confined to the kidney. Stage III: tumour extends into major veins, perinephric tissue, or regional lymph nodes — but not beyond Gerota's fascia or to distant organs. Stage IV: tumour extends beyond Gerota's fascia, invades the adrenal gland, or has spread to distant organs (lungs, bone, liver, brain). Stage directly determines the treatment approach — surgical for Stages I–III, and a combination of surgical and systemic therapy for Stage IV.
Can I get a second opinion before kidney cancer surgery?
Absolutely. CION offers a dedicated Second Opinion service in which our multidisciplinary tumour board reviews your imaging, pathology, and existing treatment recommendation before advising on the most appropriate course of action. This is particularly valuable for decisions around partial vs radical nephrectomy, active surveillance vs surgery for small renal masses, and advanced disease systemic therapy selection. A second opinion before nephrectomy is considered best oncology practice, especially when kidney-sparing surgery may be an option you have not yet been offered.
What is the latest treatment for advanced kidney cancer?
The latest standard-of-care treatments for advanced RCC are combination immunotherapy regimens approved by NCCN and supported by Phase 3 trial data. The preferred options include: nivolumab + ipilimumab (CheckMate-214) for intermediate and poor-risk disease; pembrolizumab + axitinib (Keynote-426) across all risk groups; nivolumab + cabozantinib (CheckMate-9ER); and pembrolizumab + lenvatinib (CLEAR trial). These combinations significantly outperform the previous standard of sunitinib monotherapy in overall survival and response rates. CION's medical oncology team delivers all current NCCN preferred regimens and discusses clinical trial eligibility for appropriate patients.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.