Hyderabad's Nasal & Sinus Cancer Team · NABH Accredited · 7 Locations
Nasal Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Nasal and sinus cancer — also called sinonasal cancer — is one of the rarer cancers, but when it occurs, specialist oncology management makes a critical difference to outcomes. Because the nasal cavity and sinuses sit directly beside the eyes, the brain, and major nerves, treatment requires a team experienced in both precise surgical removal and highly targeted radiation therapy that protects these structures.
Endoscopic Endonasal Surgery — minimally invasive tumour removal through the nostrils, no facial scars
4.8 · 1,000+ Google reviews · 15,000+ patients treated
7
Hyderabad Locations NABH Accredited
17+
Super-Specialist Oncologists
15,000+
Patients Treated
4.8★
Google Rating (1,000+ reviews)
Written by Dr. Gangadhar Vajrala — Radiation Oncologist · MBBS, Rangaraya Medical College, AP · MD Radiation Oncology, Kasturba Medical College, Manipal · CION Cancer Clinics, Hyderabad.
Medically Reviewed by Dr. Raghavendra Naik — Surgical Oncologist · MCh Surgical Oncology, SVIMS Tirupati · MS General Surgery, Osmania Medical College · CION Cancer Clinics, Hyderabad.
Last Medically Reviewed: May 2026
Why Nasal Cancer Is Often Diagnosed Late — And What to Watch For
The nasal cavity and sinuses sit close to the eyes and brain — which explains the unusual symptoms and why precise treatment matters.
Nasal and sinus cancer has one serious disadvantage: its early symptoms look almost exactly like a chronic sinus infection. Persistent nasal blockage, a runny nose that won't clear up, and occasional nosebleeds are easy to dismiss as sinusitis or allergies — and many patients are treated for these conditions for months before cancer is identified.
The warning signs that should prompt specialist evaluation — ideally an ENT or oncology review with nasal endoscopy and imaging — are:
Nasal blockage or stuffiness on just one side — sinusitis usually affects both sides; one-sided symptoms are more concerning.
Nosebleeds that recur without an obvious cause.
Facial pain, pressure, or numbness — particularly in one cheek or around one eye.
Swelling around the eye or cheek that wasn't there before.
Changes in vision, or double vision — a sign the tumour may be pressing on orbital structures.
Loose upper teeth or pain in the upper jaw without a dental cause.
A lump in the neck — may indicate lymph node involvement.
If you have been treated for a sinus infection that keeps coming back without fully clearing, or if any of the above signs are present for more than 4–6 weeks, ask your doctor for a nasal endoscopy. Early diagnosis is the most important factor in nasal cancer outcomes.
💡
Did You Know?
Nasal and sinus cancer symptoms closely mimic chronic sinusitis — which is why many patients receive antibiotic treatment for months before cancer is identified. The key warning sign is one-sided nasal blockage. Sinusitis typically affects both sides of the nose; one-sided, persistent obstruction that does not respond to treatment should always be investigated further.
Subtypes We Treat
Types of Nasal and Sinus Cancer We Treat
The nasal cavity is the large air-filled space directly behind the nose. The paranasal sinuses are the hollow spaces in the bones around it — the maxillary sinuses (cheekbones), ethmoid sinuses (between the eyes), frontal sinuses (above the eyes), and sphenoid sinus (deep behind the nose). Cancer can develop in any of these spaces, and the histological subtype determines treatment approach. Squamous cell carcinoma accounts for 70–80% of all nasal and sinus cancers, but several other subtypes occur. Tap any subtype to expand.
01Squamous Cell Carcinoma (SCC) — 70–80% of all cases
The most common type, accounting for 70–80% of all nasal and sinus cancers. Strongly associated with tobacco use and HPV infection. Treated with surgery followed by radiation, with or without chemotherapy. HPV-positive SCC of the sinonasal region carries a better prognosis than HPV-negative tumours — HPV testing on the biopsy specimen is therefore part of CION's standard workup.
02Adenocarcinoma — Wood & Leather Dust Exposure
The second most common type; strongly linked to occupational exposure to wood dust (carpenters, furniture makers) and leather dust (footwear industry workers) — both relevant to Hyderabad's trade workforce. Particularly common in the ethmoid sinuses. Treated with surgery + adjuvant radiation.
03Olfactory Neuroblastoma (Esthesioneuroblastoma)
A rare tumour arising near the olfactory nerve at the top of the nasal cavity. Can grow upward into the skull base. Requires combined surgical and radiation management; responds well to treatment when caught before skull base invasion. MRI is essential to define the extent of skull base involvement before surgical planning.
04Sinonasal Undifferentiated Carcinoma (SNUC)
Aggressive and rapidly growing; treated with intensive combined chemotherapy and radiation, sometimes followed by surgery. Neoadjuvant chemotherapy is often used to downstage bulky disease before definitive treatment. Multidisciplinary tumour-board review is essential for sequencing decisions.
05Adenoid Cystic Carcinoma
Slow-growing but prone to perineural spread (growing along nerves); tends to recur and requires close long-term follow-up after treatment. Adjuvant radiation is standard. Surveillance MRI for nerve-pathway recurrence is part of CION's long-term follow-up protocol for this subtype.
06Mucosal Melanoma
A rare, aggressive melanoma arising from the nasal lining; managed with surgery and radiation. Less responsive to standard melanoma systemic therapy than skin melanoma, though immunotherapy is being explored for advanced disease. Treatment is highly individualised and tumour-board led.
Differentiation
Nasal Cancer vs Nasopharyngeal Cancer — An Important Distinction
Many patients and families confuse nasal cavity cancer with nasopharyngeal cancer (NPC) — and the two are quite different diseases. Nasopharyngeal cancer develops in the nasopharynx — the upper throat, directly behind the nose. It is associated with Epstein-Barr virus (EBV) infection and is more common in Southeast Asia and parts of South India.
Nasal cavity and sinus cancer develops in the nasal passages and air spaces themselves. The two have different causes, different treatments, and different prognoses. NPC is primarily treated with radiation and chemotherapy — surgery rarely plays a role. Nasal cavity and sinus cancers are primarily treated with surgery + radiation. If you have received a diagnosis, make sure you understand which type you have — the treatment pathways are completely different.
Who is at risk
Who Is at Risk of Nasal and Sinus Cancer?
A small number of well-defined exposures account for most nasal and sinus cancers — and several of them are common in Hyderabad's industrial and trade workforce. If you are exposed to any of the following, persistent nasal symptoms should not be brushed off as 'just sinusitis'.
Tobacco use — smoking and smokeless tobacco are the primary risk factors for nasal cavity squamous cell carcinoma.
Occupational exposure to wood dust — carpenters, furniture makers, and woodworkers have a significantly elevated risk of adenocarcinoma of the ethmoid sinus; relevant for Hyderabad's furniture and carpentry workforce.
Occupational exposure to leather dust — cobbling and footwear industry workers; adenocarcinoma of the sinonasal region.
Exposure to nickel, chromium, and industrial chemicals — metal processing and electroplating workers; relevant to Hyderabad's industrial zones.
HPV infection — a subset of nasal cavity and sinus SCCs are HPV-positive, with a better prognosis than HPV-negative tumours.
Chronic sinus inflammation — long-standing, inadequately treated sinusitis is a background risk factor.
Inverted papilloma — a benign nasal polyp that can undergo malignant transformation; requires complete surgical removal and follow-up.
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Get a Free Second Opinion from CION's Nasal Cancer Team
A written second opinion from our multidisciplinary team — for diagnoses declared unresectable, or when only ENT surgery has been offered without a plan for radiation.
Diagnosis requires a combination of direct visualisation, imaging, and tissue biopsy. CION's diagnostic pathway is thorough, efficient, and aligned with NCCN and ESMO standards.
1
Nasal Endoscopy
A thin, flexible tube with a camera is passed through the nostril to directly visualise the nasal cavity and identify any suspicious lesion. Guided biopsies can be taken at the same time. This is the most important first investigation and can be done as an outpatient procedure.
2
Imaging for Staging
MRI (Magnetic Resonance Imaging) — superior for assessing soft tissue involvement, perineural spread, and orbital or skull base extension; essential for surgical planning.
CT Scan — best for assessing bone erosion and involvement of the sinus walls, skull base, and orbital bones.
PET-CT — for staging distant metastases and assessing lymph node involvement.
3
Biopsy
A tissue sample is taken from the suspicious lesion — either through nasal endoscopy or by CT-guided biopsy for deeper lesions — and sent for histopathological analysis to confirm cancer type and guide treatment planning. HPV testing is performed on biopsy tissue where appropriate, as HPV-positive tumours have a better prognosis.
TNM staging
Nasal Cancer Staging and Survival
Nasal cavity and paranasal sinus cancers are staged using the TNM system. Stage depends on tumour size, extent of local invasion into adjacent structures, and spread to lymph nodes or distant organs. Overall, early-stage cancers have much better outcomes than those detected late — reinforcing the importance of early investigation of suspicious symptoms.
Stage
Extent of Disease
Key Features
5-Year Survival
Primary Treatment
Stage I–II
Confined to nasal cavity or one sinus
No bone erosion into adjacent structures
50–70%
Surgery + adjuvant IMRT
Stage III
Invasion into adjacent sinus or bone
May involve orbital floor or ethmoid sinuses
35–50%
Surgery + adjuvant CCRT
Stage IVA
Advanced local spread
Orbital invasion, skull base, nasopharynx
20–35%
Surgery + CCRT; or definitive CCRT if unresectable
Stage IVB–C
Unresectable or distant spread
Involvement of carotid artery, brain, or metastases
10–20%
Chemoradiation ± neoadjuvant chemotherapy; palliative care
Survival estimates are for squamous cell carcinoma treated at specialist oncology centres. Adenocarcinoma and olfactory neuroblastoma may have different prognoses depending on subtype and stage.
NCCN protocol-driven
Nasal Cancer Treatment at CION Cancer Clinics
Treatment for nasal and sinus cancer almost always combines surgery and radiation therapy. Chemotherapy is added to radiation for advanced disease. Every patient's plan is reviewed by CION's multidisciplinary tumour board before treatment begins.
Surgery — Removing the Tumour
The primary goal of surgery is to remove the entire tumour with clear margins. The surgical approach depends on the tumour's size, location, and whether it has grown into adjacent structures.
Endoscopic Endonasal Surgery — the preferred approach for smaller, localised tumours confined to the nasal cavity or accessible sinuses; instruments are passed entirely through the nostrils — no external incisions, no facial scars; the camera guides precise tumour removal while preserving surrounding healthy tissue; recovery is faster than open surgery with equivalent cancer control rates for appropriate tumours.
Open Surgery (Lateral Rhinotomy, Midfacial Degloving) — for larger tumours that cannot be fully removed endoscopically; involves carefully planned incisions around the nose or inside the mouth to access the tumour; reconstruction of the affected area is planned alongside tumour removal.
Craniofacial Resection — for advanced tumours that have grown upward into the skull base; involves a combined approach through the face and skull in coordination with neurosurgical input; achieves complete tumour removal while preserving brain structures.
Maxillectomy — for tumours of the maxillary sinus that have invaded the upper jaw; partial or total removal of the upper jaw (maxilla) with prosthetic or reconstructive rehabilitation.
Neck Dissection — if the cancer has spread to lymph nodes in the neck, these are removed at the same time.
Differentiation · IMRT
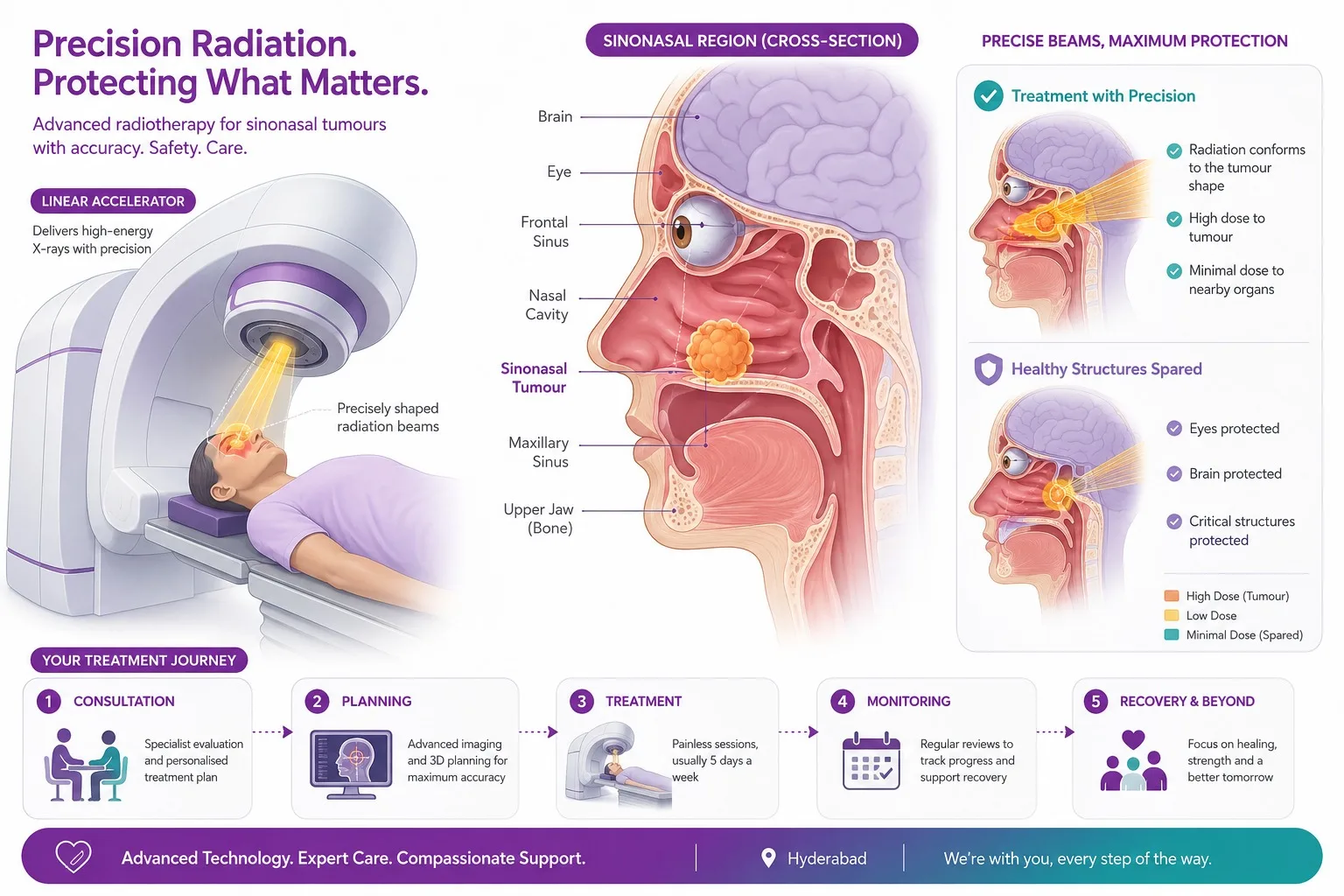
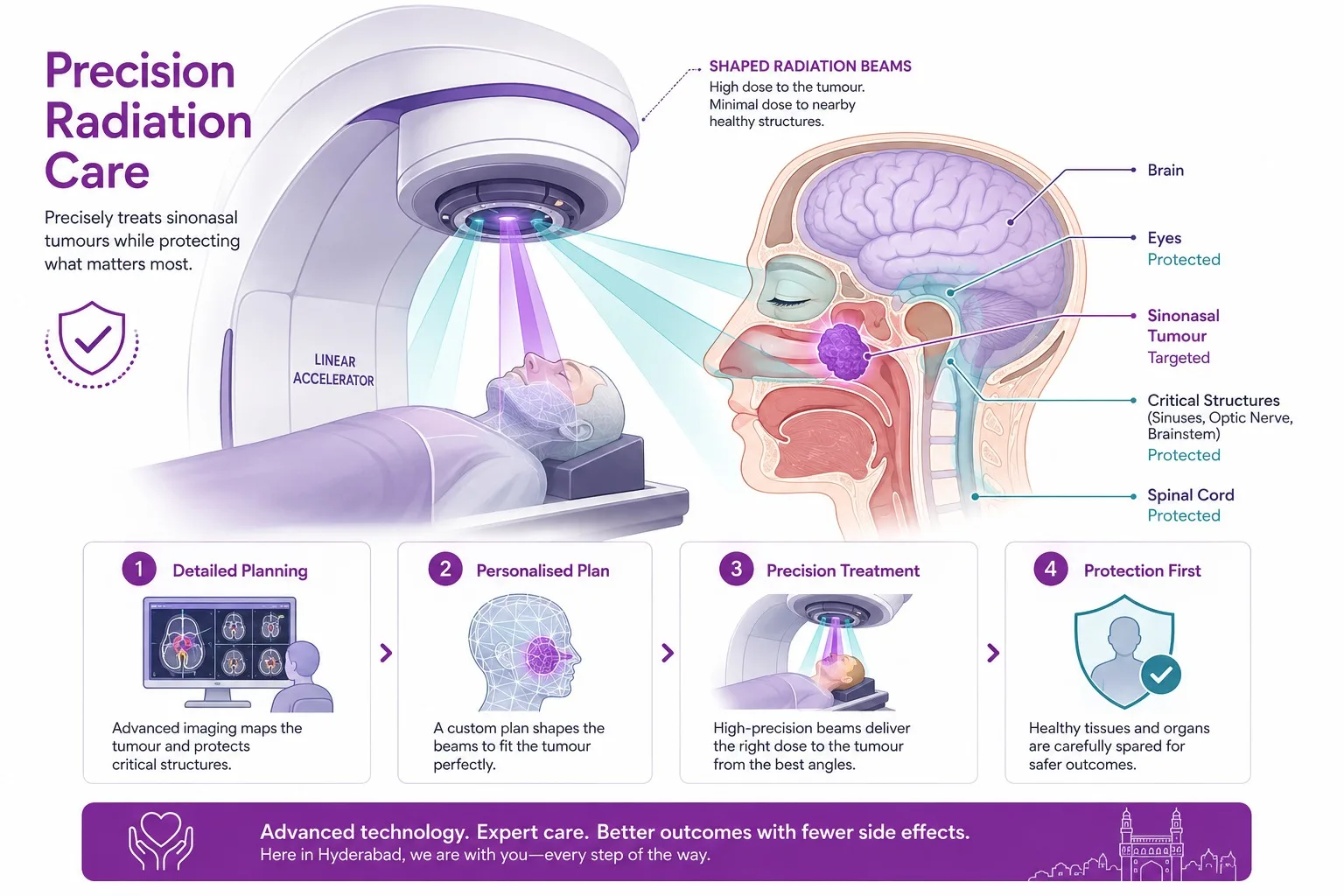
Radiation Therapy — How IMRT Protects What Matters Most
Precision radiation delivers a high dose to the tumour while sparing the eyes, optic nerves and brain nearby.
Radiation therapy after surgery is standard for most nasal and sinus cancers — but this is not straightforward radiation. The nasal cavity sits directly next to the eyes, the optic nerves, the brain, and the spinal cord. Conventional radiation to this area can damage vision and cause serious long-term complications.
This is why IMRT — Intensity-Modulated Radiation Therapy — is the standard technique for nasal and sinus cancer at CION, and why the experience of the radiation oncology team matters enormously. IMRT works by shaping the radiation beam into a precise 3D contour that matches the tumour exactly — like fitting a glove around it. High doses reach the tumour; the surrounding dose falls away sharply, significantly reducing the amount of radiation reaching the eyes, optic nerves, and brain.
Before IMRT became standard, radiation for nasal and sinus cancers carried significant risks of vision loss, dry eye, and optic nerve damage. With IMRT delivered by an experienced team, these risks are substantially reduced. CION's radiation oncology team uses IMRT with daily image guidance (IGRT) to ensure precise targeting on every treatment day.
Adjuvant IMRT (after surgery)
Given when the tumour had close or positive surgical margins, perineural invasion, or high-risk features. Typically 60–66 Gy over 6 weeks.
Definitive CCRT (unresectable disease)
IMRT radiation delivered simultaneously with cisplatin chemotherapy; chemotherapy makes cancer cells more sensitive to radiation. 70 Gy over 7 weeks.
Brachytherapy
Internal radiation placed close to the tumour; used for tumours of the nasal septum where it can be placed precisely.
Differentiation · Advanced disease
When the Cancer Is Advanced — Chemotherapy Options
For patients with locally advanced disease, chemotherapy plays two important roles alongside radiation and surgery:
Concurrent Chemotherapy with Radiation
Cisplatin — given weekly or every 3 weeks during radiation — makes cancer cells more sensitive to the radiation beam, improving local control rates. It is used for most patients with Stage III or IVA disease who undergo surgery followed by radiation, or those receiving definitive chemoradiation without surgery.
Neoadjuvant Chemotherapy — Shrinking First, Then Operating
For patients with a tumour that is technically difficult to remove completely — close to the brain, carotid artery, or both orbits — chemotherapy can be given first to shrink it before surgery is attempted. This 'neoadjuvant' approach may convert an unresectable tumour to resectable, giving the patient a chance at curative surgery that would not otherwise have been possible. ESMO guidelines support this approach for selected locally advanced cases. CION's tumour board evaluates every borderline resectable case for neoadjuvant chemotherapy before surgery.
Tumor board for every patient
Multidisciplinary Tumour Board — Every Case Reviewed
Nasal and sinus cancer is one of the most anatomically complex cancers to treat. Getting the treatment sequence right — whether to operate first or give chemotherapy first, which surgical approach to use, how to protect the orbits during radiation — requires specialist input from surgical oncology, radiation oncology, and medical oncology together. At CION, every nasal cancer case is reviewed by our multidisciplinary team before any treatment begins:
Resectability assessment — endoscopic vs open vs craniofacial approach based on MRI and CT.
Neoadjuvant chemotherapy evaluation for borderline resectable tumours.
IMRT planning with dose constraints for eyes, optic nerves, and brain.
HPV testing of biopsy tissue — HPV-positive tumours may have a better prognosis.
Orbital preservation vs exenteration decision for tumours near the eye socket.
Neck dissection evaluation based on imaging and tumour site.
NCCN protocol alignment across all histological subtypes.
Digital coordination across all 7 Hyderabad locations.
Why Choose Us
Why Patients Choose CION for Nasal Cancer Treatment in Hyderabad
Twelve reasons our patients pick CION — endoscopic surgical capability, IMRT protecting eyes and brain, neoadjuvant chemo for borderline cases, and NCCN protocols across 7 Hyderabad locations.
7 locations across Hyderabad
Kukatpally, Kompally, Ameerpet, Tolichowki, MasabTank, L.B. Nagar, Banjara Hills — close to home, no city travel
5-Star NABH Accredited
Cancer Care Institutes
NCCN & ESMO Protocol Adherence
For all sinonasal cancer subtypes — SCC, adenocarcinoma, olfactory neuroblastoma, SNUC
MCh-trained surgical oncologist
For endoscopic endonasal and open surgical resection
IMRT & IGRT radiation
With precise dose constraint planning to protect eyes, optic nerves, and brain
Neoadjuvant chemotherapy capability
For borderline resectable disease — converting inoperable to operable
Multidisciplinary tumour board
For every patient — before any treatment decision
Full integrative support
Nutrition counselling and psychological support
Dedicated Second Opinion service
Particularly for unresectable diagnoses, orbital exenteration, and ENT-only treatment plans
EMI Facility
Flexible payment options for all patients
4.8 / 5 across 1,000+ patient reviews
India's fastest-growing cancer care network — 35+ centres across Telangana & AP
15,000+ patients treated
150+ years combined oncologist experience · 17 super-specialist oncologists
Transparent Costs
Nasal Cancer Treatment Cost in Hyderabad
The cost of nasal cancer treatment in Hyderabad varies depending on the extent of surgery required and whether radiation and chemotherapy are needed. The reference ranges below are based on current Hyderabad market data. A personalised estimate is provided after your initial oncology consultation at CION.
Treatment
Approx. Cost (INR)
Notes
Endoscopic Endonasal Surgery
₹1,50,000 – ₹3,50,000
Varies by tumour extent; day or short-stay surgery
Open Surgery (Lateral Rhinotomy / Maxillectomy)
₹2,50,000 – ₹6,00,000
Complex reconstruction may add cost
Craniofacial Resection
₹4,00,000 – ₹9,00,000
Skull base involvement; neurosurgical input
IMRT Radiation (full course)
₹1,20,000 – ₹2,50,000
60–70 Gy over 6–7 weeks
Concurrent Chemoradiation (CCRT)
₹1,80,000 – ₹3,50,000
Radiation + weekly cisplatin
Full Multi-modal Treatment
₹2,50,000 – ₹10,00,000+
Depending on stage, surgical approach, and reconstruction
Costs are indicative. A personalised treatment cost estimate is provided following your initial oncology consultation at CION.
Financial Support Options
EMI Facility — flexible instalment-based payment options available for all patients.
Private Health Insurance — CION works with all major TPAs for cashless hospitalisation.
About CION Cancer Clinics
CION Cancer Clinics is India's fastest-growing cancer care network, with over 35 centres across Telangana and Andhra Pradesh. Dedicated exclusively to oncology, CION delivers NABH-accredited, NCCN and ESMO protocol-driven cancer care — bringing world-class treatment closer to patients across the region. You can see what to expect at a CION cancer centre before your first visit.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.
💡
Did You Know?
Advanced nasal and sinus cancers can grow upward through the thin bone of the skull base — making MRI essential in the staging workup. Some tumours previously declared 'unresectable' can now be operated on after neoadjuvant chemotherapy shrinks them to a resectable size. CION's tumour board reviews every borderline case for this option before treatment begins.
Take the next step
We Walk This Journey with You
Tumour board for every patient. Transparent costs. Decisions for healing, not billing.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
The most important early warning sign is one-sided nasal blockage — stuffiness or obstruction that affects only one nostril and does not respond to sinus medication. Other symptoms include: recurrent nosebleeds without an obvious cause; facial pain, pressure, or numbness (especially in one cheek or around one eye); swelling around the eye or cheek; changes in vision or double vision; loose upper teeth or pain in the upper jaw without dental cause; and a lump in the neck. Because these symptoms closely mimic chronic sinus infections, diagnosis is often delayed. Any one-sided nasal symptom lasting more than 4–6 weeks without clear improvement should be investigated with nasal endoscopy.
Is nasal cancer curable?
Yes — nasal and sinus cancer is curable, particularly when detected at an early stage. Stage I and II nasal cavity cancers treated with surgery and adjuvant radiation therapy have 5-year survival rates of 50–70%. Even Stage III disease is curable in many patients with combined surgery, radiation, and chemotherapy. Outcomes depend on tumour type, location, extent of local invasion, and the quality of treatment at a specialist oncology centre. Advanced-stage disease (Stage IV) is more challenging, but intensive multimodal treatment can achieve meaningful disease control and, in some cases, cure.
What causes nasal cancer?
The main risk factors for nasal and sinus cancer are: tobacco use — smoking and smokeless tobacco are the leading preventable causes; occupational exposure to wood dust (carpenters, furniture workers), leather dust (footwear industry workers), and industrial chemicals including nickel and chromium compounds; HPV infection (a subset of nasal SCCs are HPV-positive); and chronic sinus inflammation or an untreated inverted papilloma (a specific type of benign nasal polyp that can become cancerous). People working in carpentry, furniture manufacturing, footwear, or metal processing industries in and around Hyderabad should be aware of their elevated risk.
How is nasal cancer diagnosed?
Diagnosis begins with a nasal endoscopy — a thin camera passed through the nostril to directly visualise the nasal cavity and identify any suspicious growth. A biopsy is taken from the lesion for histopathological analysis to confirm cancer type. CT scanning assesses bone involvement and sinus wall erosion. MRI provides the most detailed picture of soft tissue extent, any spread to the orbit or skull base, and perineural invasion. PET-CT is used for staging distant spread. Together, these investigations guide both the diagnosis and the surgical and radiation treatment planning.
What is the survival rate for nasal cancer?
Survival rates vary considerably by stage and tumour type. Early-stage (Stage I/II) disease has a 5-year survival of 50–70% with specialist treatment. Stage III achieves 35–50%. Advanced disease (Stage IVA) has a 5-year survival of 20–35%. These figures reflect outcomes at specialist oncology centres delivering combined surgery, IMRT, and concurrent chemotherapy — not ENT surgery alone. The type of cancer also matters: olfactory neuroblastoma often has better outcomes than squamous cell carcinoma at the same stage; sinonasal undifferentiated carcinoma (SNUC) has a poorer prognosis. Early diagnosis is the single most important determinant of survival.
What is endoscopic nasal cancer surgery?
Endoscopic endonasal surgery removes nasal and sinus tumours entirely through the nostrils — without any external cuts or facial incisions. A thin, camera-equipped tube (endoscope) is passed through the nostril, and surgical instruments guided by the live camera image remove the tumour precisely. This minimally invasive approach has equivalent cancer control rates to traditional open surgery for appropriately selected tumours, with less blood loss, no visible scarring, a shorter hospital stay, and faster recovery. It is not suitable for all tumours — large tumours or those involving the skull base or orbit may require open or combined surgical approaches — but it is the preferred starting point for most resectable nasal and sinus cancers.
What is the difference between nasal cancer and sinus cancer?
Nasal cavity cancer develops in the large, open air space directly behind the nostrils. Sinus cancer (paranasal sinus cancer) develops in the hollow spaces in the bones around the nose — the maxillary sinuses (in the cheekbones), ethmoid sinuses (between the eyes), frontal sinuses (above the eyes), or sphenoid sinus (deep behind the nose). In practice, the two terms are often used interchangeably and are grouped together as sinonasal cancer. Both have similar risk factors, symptoms, and treatment approaches. The location of the tumour within this region affects the specific surgical approach and which structures are at risk.
Can nasal cancer spread to the brain?
Yes — advanced nasal and sinus cancers can grow upward through the thin bone of the skull base and into the anterior cranial fossa (the lowest part of the brain cavity). This is more common with olfactory neuroblastoma, sinonasal undifferentiated carcinoma, and adenoid cystic carcinoma than with squamous cell carcinoma. When skull base involvement is detected on MRI, a craniofacial resection — combining access through the face and skull — may be required to achieve complete tumour removal. This is an important reason why MRI is essential in the staging workup of all nasal and sinus cancers, and why referral to a specialist oncology centre with skull base surgical capability is important.
What is the difference between nasal cancer and nasopharyngeal cancer?
These are two completely different cancers that are often confused because of the similar names. Nasal cavity and sinus cancer develops in the nasal passages and the air spaces around the nose; it is primarily treated with surgery and radiation. Nasopharyngeal cancer (NPC) develops in the nasopharynx — the upper part of the throat, behind the nose; it is associated with Epstein-Barr virus (EBV) infection, is more common in Southeast Asia and parts of South India, and is primarily treated with radiation and chemotherapy (surgery plays little role). If you have received a diagnosis, make sure you know which type you have — the treatment approaches are fundamentally different.
Can I get a second opinion for nasal cancer treatment?
Absolutely — and for nasal cancer, a second opinion is particularly valuable given how rarely even experienced oncologists see this cancer. Key situations where a second opinion matters: if your tumour has been declared unresectable — advances in endoscopic skull base surgery and neoadjuvant chemotherapy have made some previously unresectable tumours operable; if only ENT surgery has been offered without a plan for radiation — most nasal and sinus cancers require multimodal treatment; and if the recommended approach involves eye removal or major facial reconstruction — a specialist oncology second opinion may identify less radical options. CION's multidisciplinary team offers a dedicated Second Opinion service.
Need a Second Opinion?
Free consultation with a specialist. No commitment.