NCCN & ESMO Protocol-Driven Gynae-Oncology · 7 Hyderabad Locations
Ovarian Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Outcomes in ovarian cancer depend overwhelmingly on two things: the quality of the initial surgery, and access to PARP inhibitor maintenance therapy, which has transformed long-term survival for women with BRCA-mutated and platinum-sensitive disease. CION delivers the full spectrum — from primary or interval debulking to fertility-preserving approaches, first-line carboplatin-based chemotherapy to maintenance therapy — across 7 locations, backed by NABH accreditation and NCCN protocol-driven tumour board planning.
- Debulking Surgery — Optimal cytoreduction by an experienced gynae-oncology surgical team
- PARP Inhibitor Maintenance — Olaparib / niraparib for BRCA-mutated & platinum-sensitive disease
- NACT + Interval Debulking — Structured pathway for advanced-stage patients not fit for upfront surgery
- Fertility-Preserving Surgery — For carefully selected young women · germline BRCA testing for every patient
70%
Ovarian Cancers Diagnosed
at Stage III/IV
at Stage III/IV
81.0%
1-Yr Survival Rate*
(Ovary, CION)
(Ovary, CION)
7
Hyderabad Locations
NABH Accredited
NABH Accredited
4.8★
Google Rating
(800+ reviews)
(800+ reviews)
Ovarian Cancer in Hyderabad — What You Need to Know
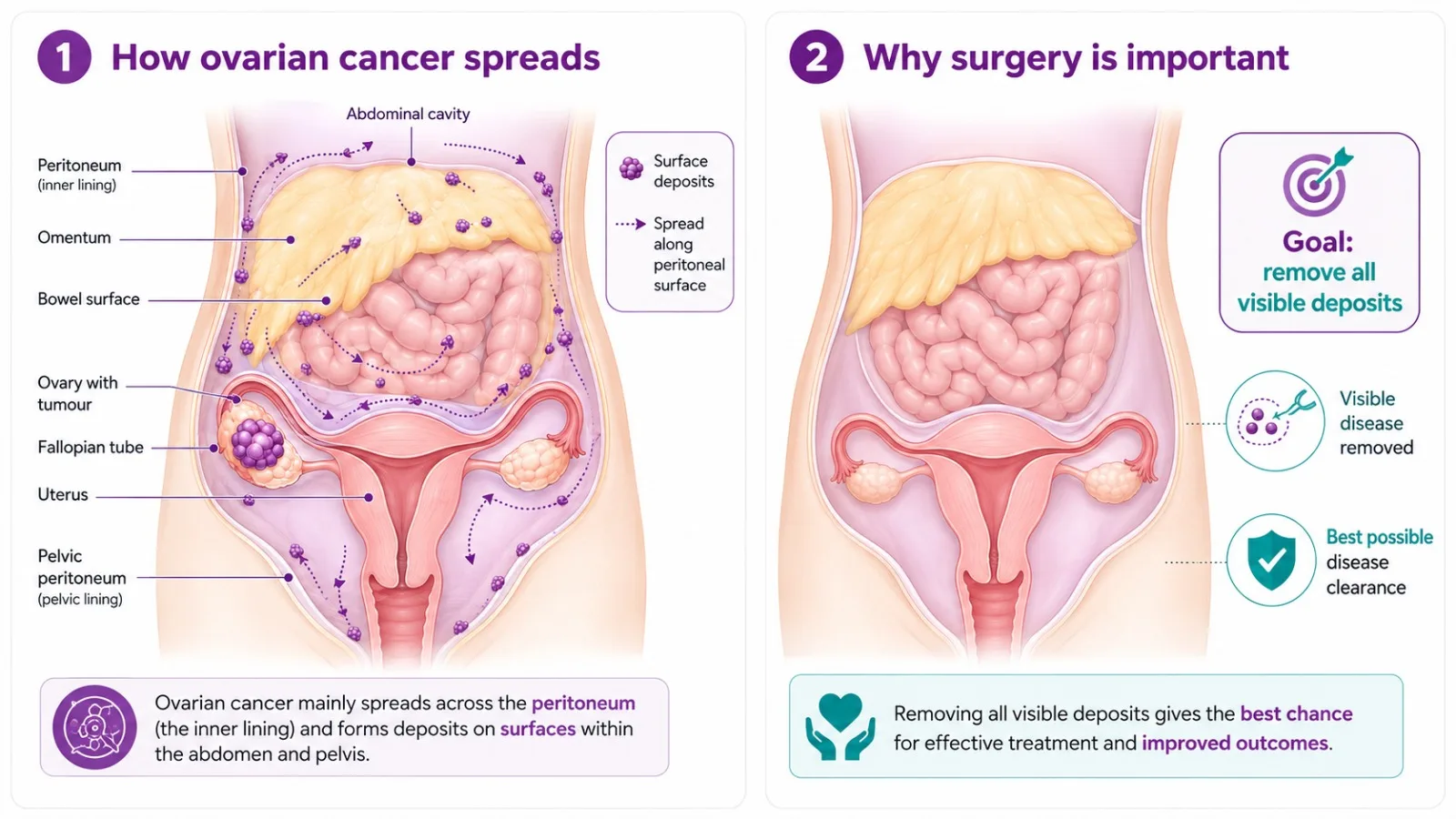
Ovarian cancer is the leading cause of gynaecological cancer death globally — not because it is the most common, but because it is so frequently diagnosed at an advanced stage. The ovaries lie deep in the pelvis, symptoms are vague and easily attributed to other conditions, and there is currently no effective population-wide screening test. Approximately 70% of women with ovarian cancer are diagnosed at Stage III or Stage IV, when the cancer has spread beyond the ovaries to the peritoneal cavity and distant organs.
In India, the median age at ovarian cancer diagnosis is under 55 — younger than in Western populations — meaning fertility preservation and hereditary risk assessment are especially relevant for Indian patients. According to the National Cancer Registry Programme (ICMR), ovarian cancer ranks among the top ten cancers in women across multiple Indian cities, with incidence rates rising in urban centres including Hyderabad.
The most important factors in ovarian cancer outcomes are: the completeness of surgical debulking (how much tumour is removed at the first operation), the quality of chemotherapy delivery, and access to maintenance therapy that delays recurrence. All three are central to CION's ovarian cancer protocol.
Did You Know? BRCA1 and BRCA2 gene mutations account for approximately 15–20% of all ovarian cancers. Current NCCN guidelines recommend germline BRCA testing for every woman diagnosed with ovarian cancer — not only those with a family history — because the results directly influence both treatment decisions and the risk assessment for family members.
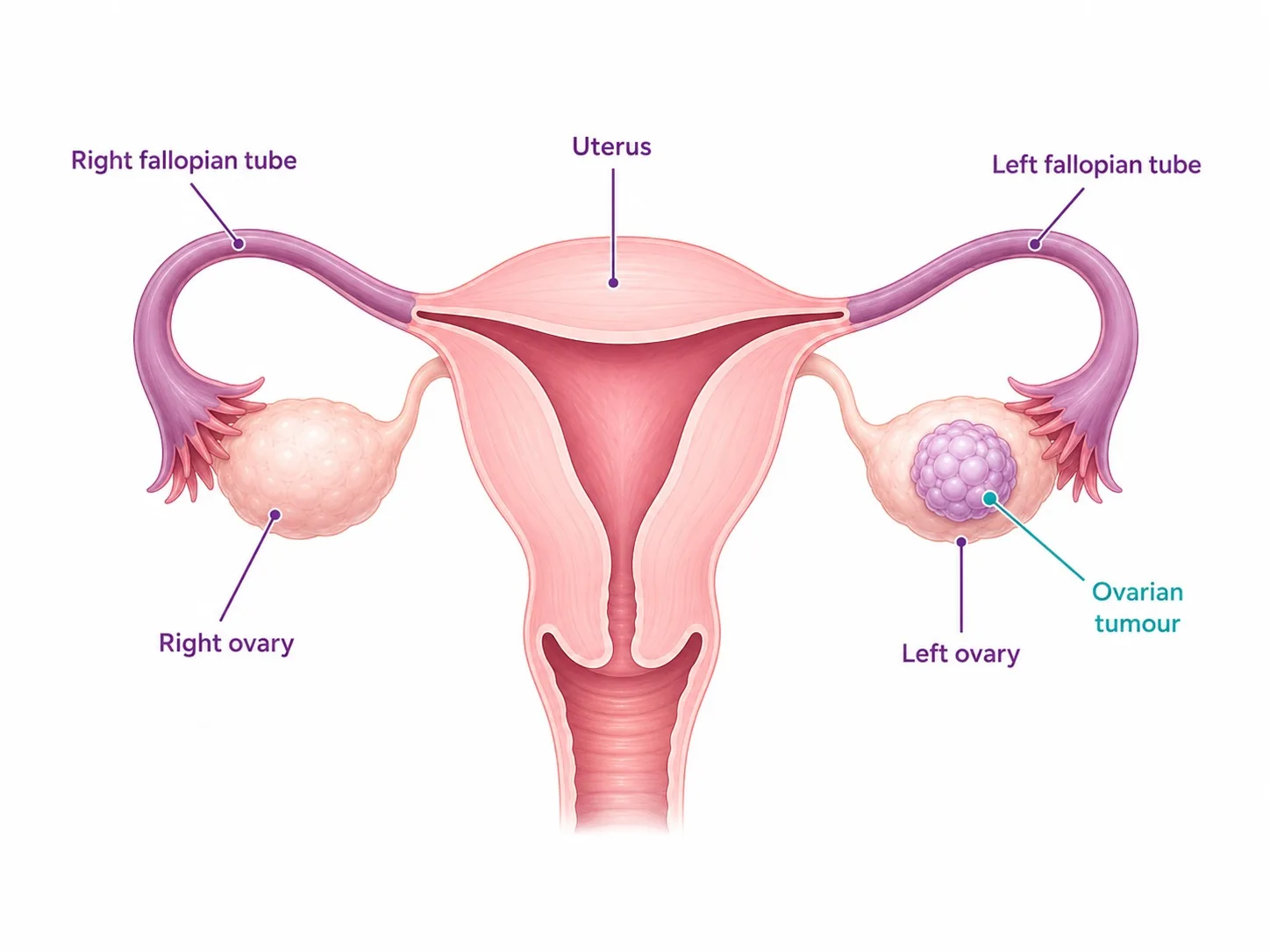
Types of Ovarian Cancer We Treat
Ovarian cancer is not one disease. At CION, our tumour board evaluates every patient's histology and molecular profile so treatment is matched to the precise subtype.
Epithelial Ovarian Cancer (EOC)
Accounts for approximately 90% of all ovarian cancers. Develops from the cells covering the outer surface of the ovary or the fallopian tube lining. Subtypes have distinct behaviour and treatment implications:
- High-Grade Serous Carcinoma (HGSC) — most common & aggressive (~70% of EOC); strongly linked to BRCA1/BRCA2; platinum-sensitive; responds well to PARP inhibitor maintenance.
- Low-Grade Serous Carcinoma (LGSC) — slower-growing; less platinum-sensitive; KRAS/BRAF-driven; often surgery + hormonal therapy.
- Clear Cell Carcinoma — associated with endometriosis; less platinum-sensitive; surgery + chemotherapy + targeted therapy in relapse.
- Endometrioid Carcinoma — linked to endometriosis & Lynch syndrome; good prognosis at early stage.
- Mucinous Carcinoma — rare; usually early stage; often misidentified as a GI primary; managed differently from serous tumours.
Germ Cell Ovarian Tumours
Arise from the egg-producing cells of the ovary. Occur predominantly in young women and adolescents. The most common malignant type is dysgerminoma, followed by immature teratoma and yolk sac tumour. Highly chemosensitive — the majority are curable even at advanced stage. Fertility-preserving surgery is the standard of care for most germ cell tumours, followed by BEP chemotherapy (bleomycin, etoposide, cisplatin) where indicated.
Sex Cord Stromal Tumours
Arise from the hormone-producing stromal cells of the ovary. Granulosa cell tumours are the most common type, often producing oestrogen and presenting with abnormal uterine bleeding. Generally slow-growing with a good prognosis at early stage. Treatment is surgical, with hormonal therapy or chemotherapy for advanced or recurrent disease. Inhibin B is a useful tumour marker for monitoring.
Symptoms of Ovarian Cancer — The Silent Disease
Ovarian cancer is frequently called a 'silent disease' — not because it produces no symptoms, but because its symptoms are vague, intermittent, and easily attributed to digestive or urinary conditions. The key is persistence: symptoms that occur more than 12 times per month and are new or more severe than usual warrant specialist evaluation. Cancer Research UK's short overview of ten things everyone should know about ovarian cancer is a helpful starting point for recognising these early warning signs.
- Persistent abdominal bloating or distension — the most common presenting symptom
- Pelvic or lower abdominal pain or pressure
- Difficulty eating or feeling full very quickly
- Frequent or urgent urination
- Unexplained weight change — loss or gain
- Changes in bowel habits — constipation, diarrhoea, or altered stool appearance
- Abnormal vaginal bleeding — particularly post-menopausal bleeding
- Fatigue and persistent tiredness
If you have experienced any of these symptoms persistently — especially if you have a family history of ovarian or breast cancer or a known BRCA mutation — consult a gynaecologic oncologist at your nearest CION location without delay.
Risk Factors for Ovarian Cancer
- BRCA1 or BRCA2 gene mutations — lifetime ovarian cancer risk of 44–46% (BRCA1) and 17–23% (BRCA2) compared to the ~1.3% population risk
- Family history of ovarian or breast cancer — particularly first-degree relatives
- Lynch syndrome (MLH1, MSH2, MSH6, PMS2 mutations) — associated with endometrioid and clear cell ovarian cancer
- Nulliparity (never having been pregnant) — each full-term pregnancy reduces risk
- Early menarche and late menopause — longer lifetime ovarian activity increases exposure
- Endometriosis — particularly associated with clear cell and endometrioid subtypes
- Hormone replacement therapy (oestrogen-only, long-term use)
- Age above 50 and postmenopausal status
- Obesity — particularly relevant in urban Hyderabad given rising rates
Protective factors include oral contraceptive use (reduces risk by up to 50% with long-term use), multiple pregnancies, and breastfeeding.
7 Centres in Hyderabad · Pick yours
CION ovarian cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centre
Beyond Hyderabad
35+ centres across Telangana & Andhra Pradesh
Travelling for treatment? We may have a centre right where you are.
Telangana
Andhra Pradesh
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.

Medical Oncologist

Medical Oncologist
Dr. C. Raghavendra Reddy
MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

Medical Oncologist
Dr. Bharati Devi Gorantla
MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

Medical Oncologist
Dr. Owais Mohammed
MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)

Medical Oncologist

Medical Oncologist

Surgical Oncologist
Dr. Muralidhar Muddusetty
MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)

Surgical Oncologist

Surgical Oncologist

Surgical Oncologist
Dr. Vinay Mamidala
MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)

Surgical Oncologist

Radiation Oncologist

Radiation Oncologist

Radiation Oncologist

Hematologist

Interventional Radiologist
Dr. Mohammed Imran

Surgical Oncologist
Dr. Vajja Sandeep Kumar
MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Surgical Oncologist
Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationBook an appointment with our specialist
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Same-week appointments across 7 Hyderabad locations
Whether you've just been diagnosed or want to understand your PARP inhibitor options — talk to a CION specialist today.
Ovarian Cancer Diagnosis at CION
Ovarian cancer cannot be definitively diagnosed without surgical tissue — but imaging and tumour markers guide the decision to operate and help plan the surgical approach. CION's diagnostic pathway is thorough and efficient.
Tumour Markers
- CA-125 — elevated in 80% of epithelial ovarian cancers; the primary tumour marker for diagnosis, treatment response monitoring, and recurrence surveillance
- HE4 (Human Epididymis Protein 4) — more specific than CA-125; used alongside CA-125 in the ROMA (Risk of Ovarian Malignancy Algorithm) score to stratify risk of malignancy in a pelvic mass
- AFP, β-hCG, LDH — tumour markers for germ cell tumours in young women
- Inhibin B — marker for granulosa cell (stromal) tumours
Imaging
- Pelvic Ultrasound (transvaginal and transabdominal) — first-line investigation; characterises ovarian mass morphology (solid vs cystic, septations, papillary projections, vascularity)
- CT Scan (chest, abdomen, pelvis) — standard staging investigation; assesses extent of peritoneal disease, lymph node involvement, and distant spread; guides surgical planning
- MRI — for characterisation of indeterminate pelvic masses; particularly useful for complex cystic lesions and assessment of local invasion
- PET-CT — for recurrent disease assessment and surveillance in selected cases
Germline BRCA Testing — Standard of Care for All Patients
NCCN guidelines now recommend germline BRCA1/BRCA2 testing for every woman diagnosed with ovarian cancer — not only those with a family history. This is because:
- BRCA mutation status directly determines eligibility for PARP inhibitor maintenance therapy — the most impactful advance in ovarian cancer treatment of the past decade
- A BRCA mutation in the patient has implications for first-degree female relatives who may wish to consider risk-reducing surgery or enhanced surveillance
- BRCA testing should be offered at diagnosis, not after chemotherapy
CION's genetic counselling service offers BRCA testing with pre- and post-test counselling for patients and their families. Somatic tumour testing for homologous recombination deficiency (HRD) is also available to identify additional patients who may benefit from PARP inhibitors beyond BRCA-mutated cases.
FIGO Staging and Survival Rates
Ovarian cancer is staged using the FIGO (International Federation of Gynecology and Obstetrics) system. Stage at diagnosis is the single strongest predictor of outcome.
| Stage | FIGO | Extent of Disease | 5-Year Survival | Primary Treatment |
|---|---|---|---|---|
| Stage I | IA–IC | Confined to one or both ovaries | 85–95% | Surgery ± chemotherapy |
| Stage II | IIA–IIC | Spread to pelvic organs (uterus, fallopian tubes) | 70–80% | Surgery + adjuvant chemotherapy |
| Stage III | IIIA–IIIC | Peritoneal spread or retroperitoneal lymph nodes | 40–60% | Debulking surgery + chemotherapy ± PARP inhibitor maintenance |
| Stage IV | IVA–IVB | Distant spread (pleural fluid, liver parenchyma, lung, groin nodes) | 15–30% | NACT → interval debulking, or systemic therapy + maintenance |
5-year survival estimates are for epithelial ovarian cancer based on international data. Individual outcomes depend on tumour grade, histological subtype, BRCA status, and completeness of surgical debulking.
CION vs National 1-Year Survival — Ovarian Cancer
Specialist tumour-board-led care, NCCN protocols, and access to PARP inhibitor maintenance translate into measurable survival differences.
CION Cancer Clinics81.0%
National average73.7%
+7.3% higher 1-year survival at CION
*1-year survival. Source: CION internal outcomes data vs ICMR National Cancer Registry Programme (NCRP).
Ovarian Cancer Treatment at CION Cancer Clinics
CION follows NCCN and ESMO protocol-driven treatment for all ovarian cancer subtypes and stages. Every case is reviewed by a multidisciplinary tumour board before treatment begins.
Surgical Oncology — Debulking and Staging
Surgery is the cornerstone of ovarian cancer management. The primary surgical goal is optimal cytoreduction — removal of all visible tumour, or at minimum reduction of residual disease to nodules under 1cm. The extent of residual disease after debulking is the single strongest predictor of survival; every millimetre matters.
- Primary Debulking Surgery (PDS) — for patients fit for upfront surgery; involves total hysterectomy, bilateral salpingo-oophorectomy (TH + BSO), omentectomy, pelvic and para-aortic lymph node sampling, peritoneal biopsies, and removal of all visible peritoneal disease including bowel, diaphragm, and spleen involvement where required
- Optimal Cytoreduction — the surgical target; no visible residual disease (R0) is ideal; residual nodules under 1cm is the minimum acceptable threshold
- Fertility-Preserving Surgery — for carefully selected young women with Stage IA, Grade 1–2 epithelial ovarian cancer, or germ cell tumours of any stage; unilateral salpingo-oophorectomy with preservation of the uterus and contralateral ovary; requires thorough staging and informed consent; discuss explicitly with your surgeon if you wish to preserve fertility
- HIPEC (Hyperthermic Intraperitoneal Chemotherapy) — heated chemotherapy delivered directly into the abdominal cavity during surgery for selected Stage III patients; administered immediately after debulking to treat microscopic peritoneal disease; available for appropriate patients at CION through coordinated surgical pathway
Chemotherapy — First-Line and Maintenance
- Carboplatin + Paclitaxel (IV) — the standard first-line regimen; administered intravenously every 3 weeks for 6 cycles; well-tolerated with manageable side effects in most patients
- Intraperitoneal (IP) Chemotherapy — carboplatin + paclitaxel delivered directly into the abdominal cavity in addition to IV chemotherapy for selected Stage III patients with optimal debulking; maximises local drug concentration at the site of microscopic peritoneal disease
- Dose-Dense Weekly Paclitaxel — alternative schedule delivering paclitaxel weekly rather than 3-weekly; demonstrated improved progression-free survival in Japanese trial data; an option for appropriate patients
- Bevacizumab (Avastin) — anti-angiogenic agent that restricts tumour blood supply; added to first-line chemotherapy and continued as maintenance therapy for Stage III/IV patients with high-risk features or Stage IV disease; NCCN recommended
Targeted Therapy and Hormonal Therapy
- Bevacizumab — anti-VEGF antibody; used as maintenance therapy after first-line chemotherapy for Stage III/IV patients, and as treatment for recurrent platinum-resistant disease
- Hormone therapy (letrozole, tamoxifen) — for low-grade serous carcinoma and selected stromal tumours that express oestrogen receptors; used as maintenance or in the recurrent setting
Radiation Therapy
Radiation therapy has a limited but important role in ovarian cancer management. CION's radiation oncology team — led by Dr. Venkata Sushma P — uses advanced techniques in specific situations:
- Palliative radiation — for symptomatic metastatic disease including bone metastases, brain metastases, or local recurrence causing pain or bleeding
- Consolidation radiation — in selected cases of localised recurrence not amenable to surgery
- IMRT and IGRT — for precise targeting when radiation is indicated, minimising bowel and bladder dose
Neoadjuvant Chemotherapy + Interval Debulking Surgery
Not every patient with advanced ovarian cancer can or should undergo primary debulking surgery upfront. For patients with extensive Stage IIIC or Stage IV disease where complete cytoreduction is not achievable at diagnosis — due to performance status, medical comorbidities, or tumour distribution — neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) is the NCCN-recommended alternative pathway.
This approach is the standard of care for a significant proportion of advanced ovarian cancer patients, yet few hospital treatment pages in Hyderabad describe it. CION's NACT + IDS pathway:
Step 1 — Multidisciplinary tumour board assessment
Review of CT imaging, CA-125, performance status, and surgical fitness to determine whether primary debulking or NACT is more appropriate.
Step 2 — Diagnostic laparoscopy (where indicated)
Minimally invasive assessment of peritoneal disease burden to confirm resectability or guide the NACT decision; avoids unnecessary laparotomy in patients where optimal debulking is not achievable.
Step 3 — Neoadjuvant chemotherapy
3 cycles of carboplatin + paclitaxel ± bevacizumab to reduce tumour burden, improve the patient's nutritional status, and create a favourable surgical window.
Step 4 — Interval Debulking Surgery (IDS)
Surgery after NACT, now targeting complete cytoreduction with a higher chance of achieving R0 than was possible at diagnosis.
Step 5 — Post-surgical chemotherapy
3 further cycles of carboplatin + paclitaxel to complete the 6-cycle course, followed by maintenance therapy assessment.
If you have been told your ovarian cancer is 'too advanced for surgery' without being offered NACT first — or if you have not been assessed by a gynaecologic oncology surgical team — request a second opinion from CION before accepting a non-surgical pathway.
PARP Inhibitor Maintenance Therapy
PARP inhibitors are one of the most impactful advances in ovarian cancer treatment of the past decade. If you have been diagnosed with ovarian cancer — particularly BRCA-mutated or platinum-sensitive disease — understanding PARP inhibitors is essential to your treatment planning.
What Are PARP Inhibitors?
PARP (Poly ADP-Ribose Polymerase) is a DNA repair enzyme. Cancer cells with BRCA mutations are already deficient in one DNA repair pathway; PARP inhibitors block a second pathway, causing cancer cell death through a mechanism called synthetic lethality. Critically, healthy cells with functioning BRCA genes can use alternative repair pathways — so PARP inhibitors are selectively toxic to BRCA-mutated cancer cells while largely sparing normal tissue.
Who Should Receive PARP Inhibitor Maintenance?
- All patients with BRCA1 or BRCA2 mutations (germline or somatic) who achieve complete or partial response to first-line platinum-based chemotherapy — olaparib maintenance is NCCN Category 1 recommended
- Patients with homologous recombination deficiency (HRD-positive tumours), regardless of BRCA mutation, who respond to platinum chemotherapy — niraparib or olaparib + bevacizumab maintenance
- All Stage III/IV patients who respond to first-line platinum chemotherapy may benefit from niraparib maintenance regardless of HRD status — NCCN recommended
How Are They Given?
PARP inhibitors (olaparib, niraparib) are oral tablets taken daily — no infusion, no hospital admission. They are typically continued for 2 years or until disease progression. Side effects include fatigue, nausea, and anaemia, all of which are manageable with monitoring and dose adjustment. CION's medical oncology team — led by Dr. N. Kiranmayee — performs regular blood count monitoring throughout PARP inhibitor maintenance.
Did You Know? The SOLO1 trial demonstrated that olaparib maintenance therapy after first-line platinum-based chemotherapy in BRCA-mutated advanced ovarian cancer improved progression-free survival by over 3 years compared to placebo. Access to PARP inhibitor maintenance at a specialist oncology centre is now one of the most important determinants of long-term outcomes in BRCA-mutated disease.
Recurrent Ovarian Cancer — Platinum-Sensitive vs Platinum-Resistant
Ovarian cancer recurs in approximately 70–80% of patients with advanced-stage disease, even after apparently successful primary treatment. Recurrence is not a treatment failure — it is a transition to a new phase of management that requires different clinical decisions. The most important distinction is the platinum-free interval (PFI) — the time between completing platinum chemotherapy and relapse:
- Platinum-sensitive recurrence (PFI >6 months) — the cancer has retained sensitivity to platinum chemotherapy; re-treatment with platinum-based chemotherapy + PARP inhibitor or bevacizumab maintenance is effective and can achieve prolonged remission
- Platinum-resistant recurrence (PFI <6 months) — the cancer no longer responds adequately to platinum; managed with non-platinum chemotherapy (gemcitabine, doxorubicin, topotecan, weekly paclitaxel), bevacizumab, and targeted agents; clinical trial enrollment should be discussed
- Platinum-refractory disease — progression during platinum chemotherapy; the most challenging clinical situation; non-platinum agents + clinical trials
CION's medical oncology team reviews every case of recurrence through the tumour board to determine the platinum-free interval, assess re-treatment options, and discuss clinical trial eligibility where appropriate.
Ovarian Cancer Treatment Cost in Hyderabad
Treatment costs vary based on stage, surgical extent, and whether systemic therapy is required. The following ranges reflect current Hyderabad market data:
| Treatment | Approx. Cost (INR) | Notes |
|---|---|---|
| Debulking Surgery (Cytoreductive) | ₹3,00,000 – ₹9,00,000 | Varies by extent; multivisceral resections at higher end |
| Staging Surgery (Early-Stage) | ₹1,50,000 – ₹3,50,000 | TH + BSO + lymph node sampling |
| Fertility-Preserving Surgery | ₹1,20,000 – ₹2,50,000 | Unilateral SO; staging biopsies additional |
| Chemotherapy — Carboplatin + Paclitaxel (per cycle) | ₹25,000 – ₹80,000 | 6 cycles standard; IP chemo at higher end |
| Bevacizumab Maintenance (per cycle) | ₹60,000 – ₹1,50,000 | Continued up to 15 months; insurance varies |
| PARP Inhibitor Maintenance (per month) | ₹50,000 – ₹1,20,000 | Olaparib / niraparib oral; may be covered under insurance |
| Full Multi-modal Treatment | ₹3,00,000 – ₹12,00,000+ | Depending on stage, sequence, and duration |
Costs are indicative. A personalised treatment cost estimate is provided after your initial oncology consultation at CION.
Financial Support Options
- EMI Facility — flexible installment-based payment options available for all patients.
- Private Health Insurance — CION works with all major TPAs for cashless hospitalisation; PARP inhibitor therapy may be covered depending on your insurer.
- Aarogyasri — empanelled for eligible Telangana residents with a White Ration Card; coverage applies to surgical and chemotherapy components subject to scheme rules.
Why Patients Choose CION for Ovarian Cancer Treatment in Hyderabad
Eighteen reasons our patients pick CION — structured NACT pathway, PARP maintenance, fertility-preserving surgery, and HIPEC.
1,000+ Ovarian cancer cases
7 locations across Hyderabad
5-Star NABH Accredited
NCCN & ESMO Protocol Adherence
NACT + Interval Debulking pathway
PARP inhibitor maintenance therapy
Germline BRCA testing at diagnosis
Fertility-preserving surgery
HIPEC coordinated
Intraperitoneal chemotherapy
Bevacizumab maintenance
Recurrent disease pathway
Full integrative support
Multidisciplinary tumour board review
Dedicated Second Opinion service
EMI facility
4.8 / 5 Google rating
35+ centres across Telangana & AP
Multidisciplinary Tumour Board — Every Case Reviewed by a Team
Ovarian cancer management requires close coordination between surgical oncology, medical oncology, radiation oncology, genetic counselling, and pathology. At CION, every ovarian cancer case is reviewed by a multidisciplinary tumour board before treatment:
- Determination of primary debulking vs NACT + IDS pathway
- Germline BRCA testing discussed and arranged at diagnosis
- Fertility preservation assessment for eligible young patients
- Intraperitoneal chemotherapy eligibility assessment after debulking
- PARP inhibitor and bevacizumab maintenance eligibility assessed after first-line chemotherapy response
- HRD testing for patients without BRCA mutation to determine extended PARP inhibitor eligibility
- Recurrence management — platinum-free interval classification and re-treatment planning
- Alignment with current NCCN and ESMO evidence-based guidelines
- Digital coordination across all 7 Hyderabad locations
Ovarian Cancer Care Near You — In Hyderabad & Beyond
CION operates 35+ centres across Telangana and Andhra Pradesh. Find your nearest gynae-oncology specialist or explore care options in your city.
Ovarian Cancer Hospitals in Hyderabad — by Location
Ovarian Cancer Care Beyond Hyderabad
Travelling for treatment? We may have a centre right where you are — across Telangana and Andhra Pradesh.
Warangal
Karimnagar
Nizamabad
Mahabubnagar
Suryapet
Nalgonda
Sangareddy
Siddipet
Vizag
Vizianagaram
Srikakulam
Bobbili
Not seeing your city? Call us — we'll connect you to the nearest CION centre or arrange a teleconsultation.
Take the First Step
Consult an ovarian cancer specialist today
If you've been told your cancer is "too advanced for surgery" without NACT being offered first — a second opinion may open a pathway that was not previously available.
Real Stories. Real Voices.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
























Read all 800+ reviews on Google
Start Your Story. Book Free Consultation.Frequently Asked Questions
Common questions about ovarian cancer treatment in Hyderabad — answered by CION's gynae-oncology team.
What are the symptoms of ovarian cancer?
The symptoms of ovarian cancer are often vague and mistaken for digestive or urinary conditions. The most important warning signs are: persistent abdominal bloating or distension (occurring more than 12 times per month), pelvic or lower abdominal pain, difficulty eating or feeling full quickly, and frequent or urgent urination. Other symptoms include unexplained weight change, changes in bowel habits, post-menopausal bleeding, and persistent fatigue. The key word is persistence — symptoms that are new, frequent, and more severe than usual warrant a specialist evaluation without delay, particularly in women over 40 or those with a family history of ovarian or breast cancer.
What is the survival rate for ovarian cancer in India?
Survival rates depend strongly on stage at diagnosis. Stage I ovarian cancer has a 5-year survival rate of 85–95% when treated at a specialist centre. Stage II: approximately 70–80%. Stage III: 40–60% — this is where PARP inhibitor maintenance therapy has made the most meaningful difference, with studies showing progression-free survival improvements of 3+ years in BRCA-mutated patients. Stage IV: 15–30%. In India, because most cases are diagnosed at Stage III or IV, early detection through awareness of symptoms and genetic risk testing makes a critical difference to individual outcomes.
Is ovarian cancer curable?
Yes — ovarian cancer is curable in a meaningful proportion of patients. Stage I and Stage II disease is curable in the majority of cases with surgery and chemotherapy. Even Stage III disease offers a genuine chance of long-term remission, particularly for patients with optimal debulking and BRCA-mutated tumours on PARP inhibitor maintenance. While Stage IV disease is rarely curable with current treatments, active management can significantly extend survival and quality of life. The most important factor is receiving care at a specialist oncology centre with the full treatment spectrum — including access to PARP inhibitors, which have transformed the prognosis for BRCA-mutated ovarian cancer.
What is debulking surgery for ovarian cancer?
Debulking surgery (also called cytoreductive surgery) is the primary surgical treatment for ovarian cancer. The goal is to remove as much tumour tissue as possible from the ovaries, fallopian tubes, uterus, omentum (fatty tissue in the abdomen), and any other involved structures including the peritoneum, bowel surface, diaphragm, and lymph nodes. The key measure of surgical success is residual disease — no visible residual tumour (R0) is the ideal outcome. Studies consistently show that the less tumour left behind after debulking, the more effective subsequent chemotherapy is and the longer the patient survives. Achieving R0 or near-R0 requires an experienced gynaecological oncology surgical team.
What is the cost of ovarian cancer treatment in Hyderabad?
Ovarian cancer treatment costs in Hyderabad vary significantly by stage and treatment pathway. Debulking surgery costs approximately ₹3,00,000 to ₹9,00,000 depending on the extent of resection. Chemotherapy cycles (carboplatin + paclitaxel) cost approximately ₹25,000 to ₹80,000 per cycle for 6 cycles. PARP inhibitor maintenance therapy (olaparib / niraparib) costs ₹50,000 to ₹1,20,000 per month and may be partially covered by private health insurance. CION provides a personalised cost estimate after your initial oncology consultation. EMI payment options are available for all patients.
What are the stages of ovarian cancer?
Ovarian cancer is staged using the FIGO system. Stage I: cancer confined to one or both ovaries — 5-year survival 85–95%. Stage II: spread to pelvic organs (uterus, fallopian tubes, bladder, or rectum) — 5-year survival 70–80%. Stage III: spread to the peritoneal lining of the abdomen or retroperitoneal lymph nodes — 5-year survival 40–60%; this is the most common stage at diagnosis in India. Stage IV: distant spread to the liver parenchyma, lungs, or distant lymph nodes — 5-year survival 15–30%. Stage at diagnosis directly determines the treatment approach and outlook.
What is a PARP inhibitor for ovarian cancer?
PARP inhibitors are oral targeted therapy tablets (olaparib/Lynparza, niraparib/Zejula) that exploit the DNA repair deficiency caused by BRCA mutations. Cancer cells with BRCA mutations rely on PARP enzymes for DNA repair; blocking PARP causes these cells to accumulate irreparable DNA damage and die. PARP inhibitors are used as maintenance therapy — taken daily for up to 2 years after a complete or partial response to platinum-based chemotherapy — to delay or prevent relapse. They are recommended by NCCN for all BRCA-mutated ovarian cancer patients and for platinum-sensitive patients with HRD-positive tumours. The SOLO1 trial showed a progression-free survival benefit of over 3 years in BRCA-mutated patients receiving olaparib maintenance.
Can ovarian cancer come back after treatment?
Yes — ovarian cancer recurs in approximately 70–80% of patients with Stage III or IV disease, even after apparently successful primary treatment. When this happens, the clinical approach depends on the platinum-free interval (PFI) — the time between finishing platinum chemotherapy and the recurrence. Patients with a PFI greater than 6 months are classified as platinum-sensitive and can often be re-treated with platinum-based chemotherapy plus PARP inhibitor or bevacizumab maintenance. Patients with a PFI under 6 months are platinum-resistant and require non-platinum agents. Recurrence is not the end of treatment — it is a transition to a new treatment phase. CION's tumour board reviews every recurrence case individually.
What is the difference between epithelial and germ cell ovarian cancer?
Epithelial ovarian cancer arises from the cells covering the outer surface of the ovary or fallopian tube lining, accounts for approximately 90% of cases, predominantly affects women over 50, and is treated with debulking surgery followed by platinum-based chemotherapy and PARP inhibitor maintenance. Germ cell ovarian tumours arise from the egg-producing cells, account for approximately 5% of cases, occur predominantly in young women and adolescents, are highly chemosensitive, and are curable in the majority of cases even at advanced stage with BEP chemotherapy. Fertility-preserving surgery is the standard of care for germ cell tumours. The two types require completely different treatment approaches — correct histological diagnosis is essential.
Can I get a second opinion before ovarian cancer surgery?
Absolutely — and for ovarian cancer, this is strongly advisable. The decision between primary debulking surgery and neoadjuvant chemotherapy first has a significant impact on surgical outcomes and quality of life; the decision on whether fertility-preserving surgery is appropriate requires specialist gynaecological oncology expertise; and PARP inhibitor eligibility requires BRCA testing that may not have been offered at every centre. CION offers a dedicated Second Opinion service where our multidisciplinary tumour board reviews your imaging, CA-125, pathology, and existing treatment recommendation before advising on the optimal pathway. If you have been told your ovarian cancer is inoperable without being assessed for NACT first, a second opinion may open a surgical pathway that was not previously offered.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.