
Pancreatic Cancer Care · 7 Hyderabad Locations
Pancreatic Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Pancreatic cancer is one of the most challenging malignancies in oncology — not because it is untreatable, but because it is rarely detected early and demands highly specialised surgical and systemic expertise. At CION Cancer Clinics, Hyderabad's dedicated oncology network, our team delivers the full spectrum of pancreatic cancer care — from complex Whipple procedures to best-in-class supportive care — across 7 locations.
- M.Ch-trained Surgical Oncologists — Whipple procedures led by Dr. Paila Gowri Naidu (M.Ch, BHU Varanasi)
- Borderline Resectable Pathway — Structured neoadjuvant chemotherapy + re-staging before surgery
- NCCN Protocol Care — Tumour-board-approved plans for PDAC, PNET, and rare pancreatic tumours
- Aarogyasri & EMI Accepted — NABH-accredited · cashless treatment for eligible patients
17+
Cancer Specialists
on Panel
on Panel
96.9%
Breast Cancer
Survival Rate*
Survival Rate*
15,000+
Patients
Treated
Treated
4.8★
Google Rating
(800+ reviews)
(800+ reviews)
Pancreatic Cancer in Hyderabad — What You Need to Know
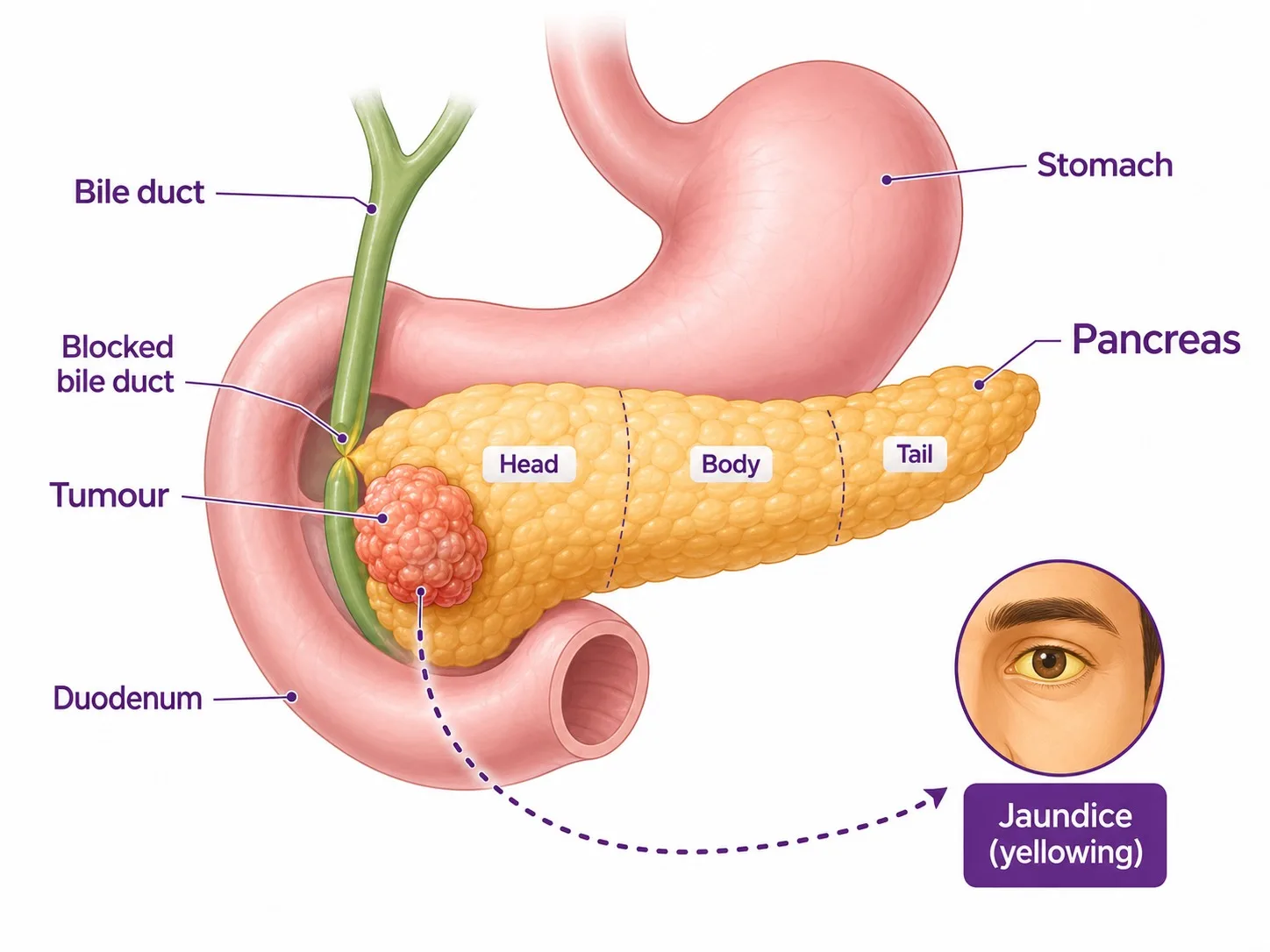
The pancreas is a dual-function organ — it produces digestive enzymes that break down food, and hormones including insulin that regulate blood sugar. Pancreatic cancer develops when cells in this organ begin to grow uncontrollably — and for a plain-language overview you can watch a Mayo Clinic specialist explain pancreatic cancer. Pancreatic ductal adenocarcinoma (PDAC) — originating in the cells lining the pancreatic ducts — accounts for approximately 93% of all pancreatic cancers. Pancreatic neuroendocrine tumours (PNETs), arising from the hormone-producing cells, comprise the remaining 7% and carry a significantly different, generally more favourable prognosis.
The primary challenge with pancreatic cancer is late presentation — approximately 80% of patients are diagnosed at Stage III or Stage IV, when the cancer has either involved major blood vessels or spread to distant organs. However, even in advanced stages, carefully managed chemotherapy, radiation, and supportive care can meaningfully extend life and preserve quality of life. For the roughly 20% of patients diagnosed at an earlier stage, surgery offers a genuine chance of cure.
Hyderabad's rising rates of type 2 diabetes, obesity, and chronic pancreatitis — all significant risk factors for PDAC — make early awareness and specialist access increasingly important across the city.
Did You Know? New-onset diabetes in adults over 50 with no obvious risk factors — particularly when accompanied by unexplained weight loss — can be an early warning sign of pancreatic cancer. If you or a family member has recently developed diabetes without a clear cause, a specialist evaluation including pancreatic imaging is advisable.
Types of Pancreatic Cancer We Treat
Pancreatic cancer is not one disease. The histological type — adenocarcinoma versus neuroendocrine versus rare subtypes — determines prognosis, treatment, and the specialists you need. CION's tumour board confirms the exact type for every patient before any treatment decision.
~93% of cases
Pancreatic Ductal Adenocarcinoma (PDAC)
The most common and most aggressive form. PDAC arises in the ductal cells lining the pancreatic ducts. It is characterised by early vascular invasion, perineural spread, and resistance to many systemic therapies. Most PDACs arise in the head of the pancreas (60–70%), causing biliary obstruction and jaundice; tumours in the body or tail tend to present later, when they are larger and more advanced. Treatment depends on resectability status — the single most important determinant of the treatment pathway.
~7% of cases
Pancreatic Neuroendocrine Tumours (PNETs)
PNETs arise from the hormone-producing islet cells of the pancreas and behave very differently from PDAC — typically slower-growing, more amenable to surgery, and responsive to distinct systemic therapies including somatostatin analogues (octreotide, lanreotide), everolimus, and sunitinib. PNETs are classified as functioning (insulinoma, glucagonoma, gastrinoma, VIPoma) or non-functioning. Five-year survival for well-differentiated Grade 1 and Grade 2 tumours is significantly better than PDAC.
Rare subtypes
Rare Pancreatic Tumours
Less common pancreatic tumours include acinar cell carcinoma, solid pseudopapillary neoplasms (typically in young women, generally low malignant potential), mucinous cystic neoplasms (MCNs), intraductal papillary mucinous neoplasms (IPMNs — which carry a risk of malignant transformation), and ampullary carcinoma (at the junction of the bile duct and pancreatic duct, with generally better prognosis than PDAC). CION's tumour board manages all rare pancreatic tumour types through an individualised protocol.
Risk Factors for Pancreatic Cancer
Several factors increase the risk of developing pancreatic cancer. Many are modifiable; others — like family history and inherited gene mutations — guide screening decisions. Discuss your personal risk profile with a CION specialist if more than one applies to you.
- Smoking — doubles the risk of PDAC; one of the most modifiable risk factors
- Chronic pancreatitis — long-standing pancreatic inflammation significantly raises PDAC risk
- Type 2 diabetes — particularly new-onset diabetes in older adults without traditional risk factors
- Obesity — especially central/abdominal obesity, increasingly prevalent in urban Hyderabad
- Family history of pancreatic cancer — first-degree relatives carry 2–3 times higher risk
- Hereditary gene mutations — BRCA1/BRCA2, PALB2, ATM, CDKN2A, MLH1/MSH2 (Lynch syndrome); account for approximately 10% of PDAC cases
- Long-standing chronic pancreatitis from any cause (gallstones, alcohol, autoimmune)
- Age above 60 — most cases occur in the sixth to eighth decade
Symptoms of Pancreatic Cancer
Pancreatic cancer is frequently called a 'silent disease' — symptoms are often absent or non-specific in early stages, which is why most cases are diagnosed late. The following symptoms warrant urgent specialist evaluation:
- Painless jaundice — yellow skin and eyes, dark urine, pale stools; caused by bile duct obstruction from a tumour in the head of the pancreas; the most actionable early warning sign
- Upper abdominal pain radiating to the mid-back — often worse when lying down, improves leaning forward
- Unexplained significant weight loss and loss of appetite
- New-onset diabetes or sudden worsening of previously well-controlled blood sugar
- Nausea, vomiting, and feeling of fullness after small meals
- Pale, greasy, or floating stools (steatorrhoea) — indicating fat malabsorption from pancreatic enzyme deficiency
- Fatigue and general weakness
- Blood clots in unusual locations (deep vein thrombosis) — a paraneoplastic manifestation sometimes preceding diagnosis
Painless jaundice in any adult is a red flag that requires same-week imaging and specialist review. Do not wait. Book a consultation with a pancreatic cancer specialist at your nearest CION location.
Why Patients Choose CION for Pancreatic Cancer Treatment in Hyderabad
Sixteen reasons our patients pick CION — across surgical expertise, structured borderline-resectable pathway, targeted therapy, and palliative care.
1,000+ cancer cases
7 locations across Hyderabad
5-Star NABH Accredited
NCCN Protocol Adherence
M.Ch-trained surgical oncologist
Borderline resectable pathway
EUS-guided biopsy
PNET-specific treatment pathway
Olaparib targeted therapy
Comprehensive palliative & supportive care
Multidisciplinary tumour board review
Dedicated Second Opinion service
Aarogyasri empanelled
EMI facility
4.8 / 5 Google rating
35+ centres across Telangana & AP
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.






Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centre
Beyond Hyderabad
35+ centres across Telangana & Andhra Pradesh
Travelling for treatment? We may have a centre right where you are.
Telangana
Andhra Pradesh
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.

Medical Oncologist

Medical Oncologist
Dr. C. Raghavendra Reddy
MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

Medical Oncologist
Dr. Bharati Devi Gorantla
MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

Medical Oncologist
Dr. Owais Mohammed
MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)

Medical Oncologist

Medical Oncologist

Surgical Oncologist
Dr. Muralidhar Muddusetty
MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)

Surgical Oncologist

Surgical Oncologist

Surgical Oncologist
Dr. Vinay Mamidala
MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)

Surgical Oncologist

Radiation Oncologist

Radiation Oncologist

Radiation Oncologist

Hematologist

Interventional Radiologist
Dr. Mohammed Imran

Surgical Oncologist
Dr. Vajja Sandeep Kumar
MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Surgical Oncologist
Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationBook an appointment with our specialist
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Ready to Speak with a Pancreatic Cancer Oncologist?
You don't have to navigate a pancreatic cancer diagnosis alone. Our oncologists are available across 7 Hyderabad locations with same-week appointments and a dedicated borderline-resectable pathway.
Pancreatic Cancer Diagnosis at CION
An accurate diagnosis that establishes both the histological type and resectability status is essential before any treatment decision. CION's diagnostic pathway integrates imaging, endoscopy, and molecular testing.
Imaging
- CT Scan (multiphasic, pancreatic protocol) — the gold standard first-line imaging investigation; defines tumour size, location, involvement of major vessels (superior mesenteric artery/vein, portal vein, coeliac axis), and distant spread; determines resectability
- MRI / MRCP — used for biliary anatomy assessment, liver lesion characterisation, and when CT findings are indeterminate
- PET-CT — for staging and detection of distant metastases not visible on CT; used selectively in borderline resectable cases before surgery
Endoscopic Ultrasound (EUS) — The Diagnostic Gold Standard
EUS is the most sensitive imaging modality for small pancreatic tumours and the standard method for obtaining tissue diagnosis. A thin flexible scope with an ultrasound probe is passed through the mouth to the stomach and duodenum, allowing real-time, high-resolution imaging of the pancreas from inside the gastrointestinal tract. EUS-guided fine needle aspiration (FNA) or fine needle biopsy (FNB) obtains tissue for histological confirmation without the risks of percutaneous biopsy. CION's diagnostic pathway includes EUS for all cases where tissue confirmation is required before treatment — a capability that distinguishes CION from centres that rely solely on CT-guided biopsy.
Blood Tests
- CA19-9 tumour marker — elevated in the majority of PDAC cases; used for diagnosis support, treatment response monitoring, and surveillance after surgery
- Liver function tests — assess biliary obstruction severity and fitness for surgery
- Germline genetic testing — for BRCA1/BRCA2, PALB2, and other hereditary mutations; influences systemic therapy eligibility (olaparib for BRCA-mutated advanced PDAC) and guides family screening
Pancreatic Cancer Staging and Resectability
Pancreatic cancer staging is determined by TNM classification, but the clinically critical categorisation is resectability status — which directly determines the treatment pathway. CION's tumour board assesses resectability using the high-quality CT imaging and the criteria outlined below.
| Stage | Resectability | Tumour Status | Primary Treatment Approach |
|---|---|---|---|
| Stage I | Resectable | Confined to pancreas, no vascular involvement | Upfront surgery (Whipple / distal pancreatectomy) + adjuvant chemotherapy |
| Stage II | Resectable / Borderline | Extends beyond pancreas; may abut (but not involve) major vessels | Upfront surgery if fully resectable; neoadjuvant chemotherapy if borderline — reassess for surgery |
| Stage III | Locally Advanced / Unresectable | Involves major vessels (SMA, coeliac); no distant metastasis | Chemotherapy ± chemoradiation; reassess resectability after response |
| Stage IV | Metastatic | Spread to liver, lungs, peritoneum or distant organs | Systemic chemotherapy + supportive care; palliative surgery where needed for obstruction |
All staging and resectability assessments are performed by CION's multidisciplinary tumour board. The categorisation above reflects NCCN criteria and is subject to individual patient factors including performance status, liver function, and comorbidities.
Borderline Resectable Pancreatic Cancer — What It Means and How CION Approaches It
Borderline resectable pancreatic cancer is one of the most important — and most misunderstood — diagnoses in oncology. It refers to tumours that abut (touch) but do not clearly encase major blood vessels such as the superior mesenteric artery (SMA), superior mesenteric vein (SMV), portal vein, or coeliac axis. These tumours cannot be removed with clear surgical margins in their current state — but with the right pre-surgical treatment, they may become resectable.
Most hospital treatment pages in Hyderabad do not address borderline resectable disease — leaving patients who receive this diagnosis without a clear local pathway. CION manages borderline resectable pancreatic cancer through a structured neoadjuvant approach:
-
1
Multidisciplinary tumour board review
Confirm borderline resectable status with high-quality pancreatic protocol CT; assess performance status and fitness for chemotherapy.
-
2
Neoadjuvant chemotherapy
4–6 months of systemic chemotherapy (gemcitabine + nab-paclitaxel or FOLFIRINOX regimen depending on patient fitness) to shrink the tumour and create a margin around blood vessels.
-
3
Re-staging imaging
Repeat CT scan after neoadjuvant therapy to assess response and determine whether the tumour has been downstaged to resectable.
-
4
Surgery
If re-staging confirms adequate response and resectable margins, proceed to Whipple procedure or distal pancreatectomy; vascular resection and reconstruction performed where required.
-
5
Post-surgical adjuvant therapy
Additional chemotherapy following surgery to reduce recurrence risk.
Not all borderline resectable patients will ultimately proceed to surgery — but every borderline resectable patient deserves a structured attempt at curative treatment. If you have been told your pancreatic cancer 'might be operable' or is 'close to the blood vessels,' ask for a second opinion from CION's tumour board before accepting a non-surgical pathway.
Pancreatic Cancer Treatment at CION Cancer Clinics
CION follows NCCN protocol-driven treatment planning for all pancreatic cancer subtypes and stages. Every case is reviewed by a multidisciplinary tumour board before treatment begins.
Surgical Oncology — Pancreatic Cancer Surgery
Surgery is the only potentially curative treatment for pancreatic cancer. CION's surgical oncology team, led by Dr. Paila Gowri Naidu (M.Ch Surgical Oncology, BHU Varanasi) and Dr. Sridhar Kamani (DrNB Surgical Oncology), performs the full range of pancreatic resections.
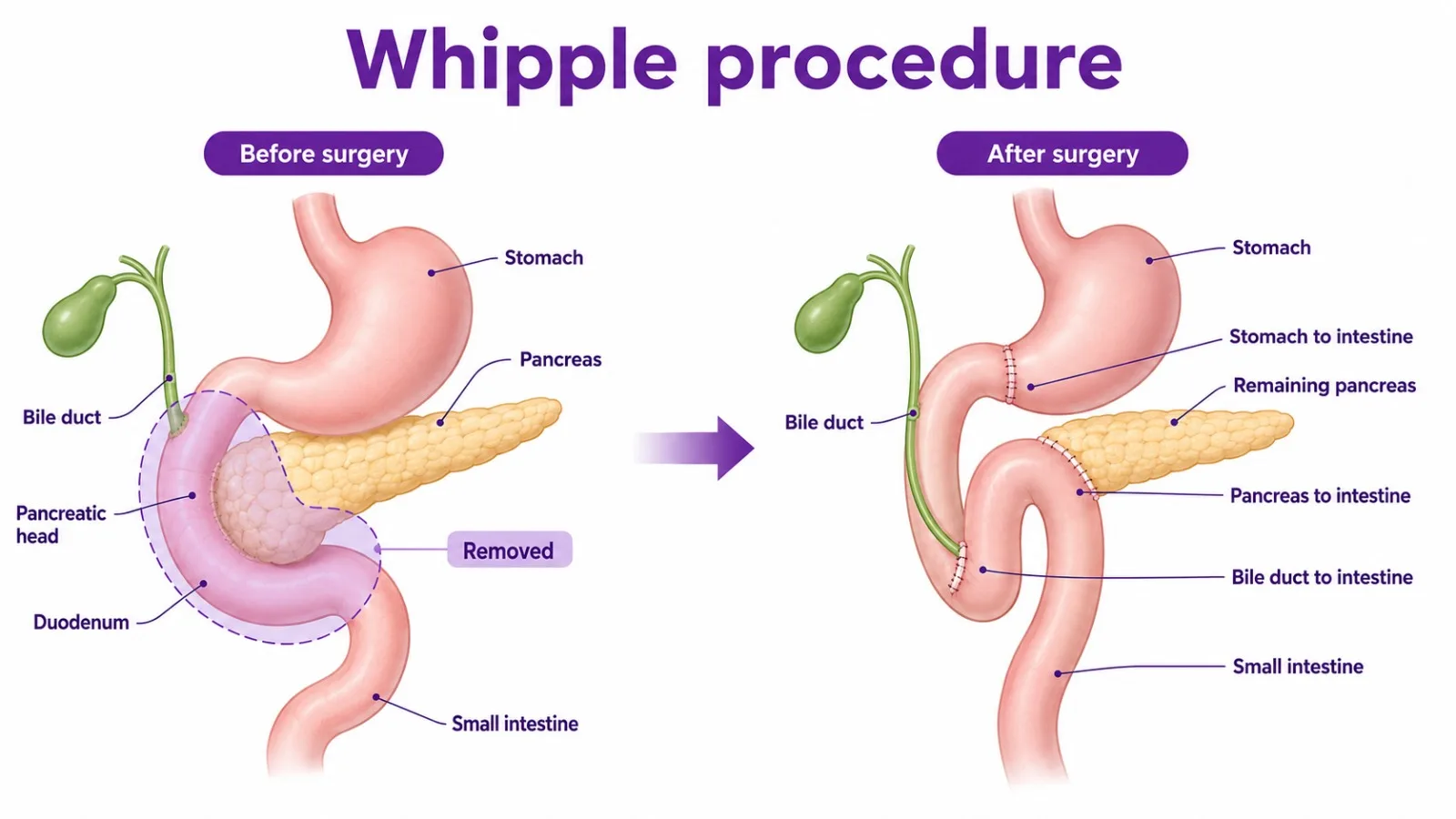
- Whipple Procedure (Pancreaticoduodenectomy) — the gold standard surgery for cancers in the head of the pancreas. One of the most complex abdominal operations in oncology, involving removal of the head of the pancreas, the duodenum, gallbladder, part of the bile duct, and sometimes part of the stomach. Performed in a dedicated hepatopancreaticobiliary surgical setting with ICU support.
- Distal Pancreatectomy — removal of the body and tail of the pancreas, usually with the spleen, for tumours in these locations. Can be performed open or laparoscopically in carefully selected patients.
- Total Pancreatectomy — removal of the entire pancreas, duodenum, bile duct, gallbladder, and spleen. Indicated for diffuse or multifocal tumours. Requires lifelong insulin therapy and pancreatic enzyme replacement.
- Palliative Surgical Bypass — for patients with advanced disease causing biliary obstruction (jaundice) or gastric outlet obstruction; surgical bypass (hepaticojejunostomy, gastrojejunostomy) relieves obstruction and improves quality of life.
Chemotherapy — Neoadjuvant, Adjuvant, and Palliative
Chemotherapy is used at every stage of pancreatic cancer management. CION's medical oncology team delivers current NCCN preferred regimens in a comfortable day-care setting.
- Neoadjuvant Chemotherapy (before surgery) — for borderline resectable and locally advanced disease; aims to downstage the tumour and improve the chance of achieving clear surgical margins
- Adjuvant Chemotherapy (after surgery) — recommended for all resected pancreatic cancer patients for 6 months post-surgery per NCCN guidelines; significantly reduces recurrence risk
- Palliative Chemotherapy (for advanced/metastatic disease) — improves survival and quality of life; NCCN preferred regimens include gemcitabine + nab-paclitaxel and modified FOLFIRINOX for fit patients
- Targeted Therapy (Olaparib) — PARP inhibitor, NCCN-recommended maintenance therapy for patients with advanced PDAC and germline BRCA1/BRCA2 mutations whose disease has not progressed on platinum-based chemotherapy; CION's genetic counselling service identifies eligible patients
Radiation Therapy
CION's radiation oncology team uses advanced, precisely targeted techniques for pancreatic cancer:
- Chemoradiation (concurrent chemotherapy + radiation) — for locally advanced, unresectable Stage III pancreatic cancer; chemotherapy sensitises cancer cells to radiation, improving local control
- Stereotactic Body Radiation Therapy (SBRT) — high-dose, precisely targeted radiation delivered in a small number of fractions; an option for locally advanced disease not responding to chemotherapy, or for patients not fit for surgery
- IMRT (Intensity-Modulated Radiation Therapy) — used to deliver therapeutic doses to the pancreatic tumour while protecting the duodenum, stomach, kidneys, and spinal cord
- Palliative radiation therapy — for pain control from local tumour invasion or bone metastases
Pancreatic Neuroendocrine Tumour (PNET) Treatment in Hyderabad
PNETs are fundamentally different from PDAC in their biology, behaviour, and treatment — yet most hospital treatment pages in Hyderabad fail to address them. If you have been diagnosed with a PNET rather than pancreatic adenocarcinoma, your prognosis, treatment options, and the specialists you need are different.
- Surgery — the preferred treatment for resectable PNETs of any grade; even metastatic PNETs may benefit from debulking surgery to control hormonal symptoms and prolong survival
- Somatostatin Analogues (octreotide LAR, lanreotide) — for functioning PNETs to control hormonal symptoms and inhibit tumour growth in Grade 1 and Grade 2 tumours
- Everolimus (mTOR inhibitor) — approved for progressive, well-differentiated PNETs; significantly improves progression-free survival
- Sunitinib (TKI) — approved for well-differentiated pancreatic NETs; used for progressive disease
- Peptide Receptor Radionuclide Therapy (PRRT) — for somatostatin receptor-positive PNETs; a specialised treatment coordinated through CION's referral network
- Chemotherapy — for high-grade (Grade 3) poorly differentiated pancreatic NETs, which behave more like PDAC and are treated with platinum-based regimens
Palliative and Supportive Care — Central to Pancreatic Cancer Management
Approximately 80% of pancreatic cancer patients present at Stage III or Stage IV, when curative surgery is not possible. This does not mean that nothing can be done — it means that the goals of care shift to controlling the disease, relieving symptoms, maintaining nutritional status, and preserving quality of life for as long as possible. CION's palliative care approach for pancreatic cancer is a substantive, integrated pathway — not an afterthought:
- Biliary drainage — for patients with obstructive jaundice, endoscopic biliary stenting or surgical bypass relieves jaundice, itching, and liver impairment; improves tolerance of chemotherapy
- Pain management — specialist pain management including coeliac plexus neurolysis (nerve block) for intractable pancreatic pain; a procedure that can provide months of meaningful pain relief
- Pancreatic enzyme replacement therapy (PERT) — vital for maintaining nutritional absorption; pancreatic exocrine insufficiency is near-universal in advanced PDAC
- Nutritional support — dietitian-led guidance to maintain weight and strength during chemotherapy; high-calorie, easily digestible nutrition plans tailored to each patient
- Psychological support — psycho-oncology counselling for patients and families; managing the emotional impact of a pancreatic cancer diagnosis requires dedicated support
- Insulin management — for patients with diabetes arising from pancreatic destruction or total pancreatectomy
- Ascites management — drainage (paracentesis) for patients with advanced disease and symptomatic fluid accumulation
At CION, every Stage III and Stage IV pancreatic cancer patient has a dedicated supportive care plan established alongside their oncology treatment — because managing this disease well means managing the whole patient, not just the tumour.
Multidisciplinary Tumour Board — Every Case Reviewed by a Team
Pancreatic cancer requires one of the most complex multidisciplinary decisions in oncology — particularly for borderline resectable disease, where the choice between immediate surgery and neoadjuvant chemotherapy first can determine whether a patient ever reaches the operating table. At CION, every pancreatic cancer case is reviewed by a tumour board before any treatment decision:
- Resectability assessment using standardised NCCN criteria on high-quality pancreatic protocol CT
- Performance status and liver function evaluation for chemotherapy and surgical fitness
- Germline genetic testing (BRCA/PALB2) discussed for all patients — to assess targeted therapy eligibility
- Neoadjuvant vs upfront surgery decision for borderline resectable cases
- Biliary drainage planning before chemotherapy for jaundiced patients
- PNET vs PDAC pathway differentiation based on histology and grade
- Palliative care plan established from diagnosis for Stage III/IV patients
- Digital coordination across all 7 Hyderabad locations for uninterrupted care
Did You Know? The addition of nab-paclitaxel to gemcitabine (the MPACT trial) improved median overall survival from 6.7 to 8.5 months in advanced pancreatic cancer — a meaningful improvement in a disease with historically very limited systemic treatment options. Access to current NCCN-approved regimens at a specialist centre is the most important determinant of outcomes in advanced disease.
Pancreatic Cancer Treatment Cost in Hyderabad
Pancreatic cancer treatment costs vary significantly based on stage, resectability, and whether surgery, chemotherapy, or palliative care is the primary pathway. The following ranges are based on current Hyderabad market data:
| Treatment | Approx. Cost (INR) | Notes |
|---|---|---|
| Whipple Procedure (Pancreaticoduodenectomy) | ₹4,00,000 – ₹12,00,000 | Complex surgery; varies by ICU stay and complications |
| Distal Pancreatectomy | ₹3,00,000 – ₹8,00,000 | Open or laparoscopic; includes splenectomy in most cases |
| Total Pancreatectomy | ₹5,00,000 – ₹14,00,000 | Higher cost; lifelong insulin/enzyme replacement required |
| Chemotherapy (per cycle) | ₹20,000 – ₹1,50,000 | Gemcitabine-based regimens at lower end; combination regimens higher |
| Chemoradiation (full course) | ₹1,50,000 – ₹3,50,000 | Concurrent chemotherapy + radiation for locally advanced disease |
| Biliary Stenting / Drainage | ₹30,000 – ₹1,00,000 | Endoscopic or surgical; for obstructive jaundice |
| Full Multi-modal Treatment | ₹3,00,000 – ₹15,00,000+ | Depending on stage, treatment sequence, and duration |
Costs are indicative. A personalised treatment cost estimate is provided following your initial oncology consultation at CION.
Financial Support Options
- Aarogyasri Scheme — cashless treatment coverage for eligible Telangana residents (White Ration Card holders). CION is Aarogyasri empanelled.
- EMI Facility — flexible instalment-based payment options available for all patients.
- Private Health Insurance — CION works with all major TPAs for cashless hospitalisation.
Pancreatic Cancer Care Near You — In Hyderabad & Beyond
CION operates 35+ centres across Telangana and Andhra Pradesh. Find your nearest pancreatic cancer specialist or explore care options in your city.
Pancreatic Cancer Care in Hyderabad — by Location
Pancreatic Cancer Care Beyond Hyderabad
Travelling for treatment? We may have a centre right where you are — across Telangana and Andhra Pradesh.
Vizag
Warangal
Karimnagar
Nizamabad
Mahabubnagar
Suryapet
Nalgonda
Sangareddy
Siddipet
Vizianagaram
Srikakulam
Bobbili
Not seeing your city? Call 18002028726 — we'll connect you to the nearest CION centre or arrange a teleconsultation.
Second Opinion Available
Get a Free Written Second Opinion from CION's Tumour Board
Our multidisciplinary team reviews your imaging, pathology, and existing treatment plan — before you commit to Whipple surgery or chemotherapy.
Real Stories. Real Voices.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
























Read all 800+ reviews on Google
Start Your Story. Book Free Consultation.Frequently Asked Questions — Pancreatic Cancer Treatment
Common questions about pancreatic cancer treatment in Hyderabad — answered by CION's oncology team.
What is the best treatment for pancreatic cancer?
The best treatment depends entirely on stage and resectability. For the approximately 20% of patients with resectable disease, surgery — typically the Whipple procedure for head-of-pancreas tumours — followed by 6 months of adjuvant chemotherapy offers the best chance of cure. For borderline resectable disease, neoadjuvant chemotherapy to downstage the tumour before surgery is the current NCCN-preferred approach. For advanced (Stage III/IV) disease, combination chemotherapy with gemcitabine + nab-paclitaxel or FOLFIRINOX is the standard of care, alongside comprehensive supportive care. CION's multidisciplinary tumour board determines the most appropriate pathway for every individual patient.
What is the cost of pancreatic cancer treatment in Hyderabad?
Costs vary significantly by stage and treatment pathway. The Whipple procedure costs approximately ₹4,00,000 to ₹12,00,000 depending on ICU stay and complications. Chemotherapy cycles range from ₹20,000 to ₹1,50,000 depending on the regimen. Chemoradiation for locally advanced disease costs approximately ₹1,50,000 to ₹3,50,000. Biliary stenting for jaundice relief costs ₹30,000 to ₹1,00,000. A personalised estimate is provided after your initial CION consultation. Aarogyasri and EMI payment options are available.
Is pancreatic cancer curable?
Yes — for the approximately 20% of patients diagnosed with early-stage, resectable disease, surgery followed by adjuvant chemotherapy offers a genuine chance of cure, with five-year survival rates of 20–30% after complete resection. For borderline resectable disease, neoadjuvant chemotherapy followed by surgery can achieve cure in a meaningful proportion of patients who respond well. For the majority who present at advanced stage, cure is not achievable with current treatments — but active management with chemotherapy can significantly extend life and maintain quality of life. Early detection and specialist evaluation the moment symptoms appear is the most important step.
What are the early signs of pancreatic cancer?
The most actionable early warning signs are: painless jaundice (yellowing of skin and eyes with dark urine and pale stools) — this should trigger same-week imaging; new-onset diabetes in adults over 50 without typical risk factors, especially with weight loss; unexplained significant weight loss; and persistent upper abdominal or mid-back pain not explained by other conditions. Because the pancreas is deep in the abdomen and symptoms are often non-specific, most early signs are subtle. If you have any risk factors for pancreatic cancer — particularly chronic pancreatitis, a family history, or BRCA/PALB2 mutations — discuss surveillance with a specialist.
What is the Whipple procedure?
The Whipple procedure (pancreaticoduodenectomy) is the standard surgery for resectable pancreatic cancer located in the head of the pancreas. It involves removal of the head of the pancreas, the duodenum (first part of the small intestine), the gallbladder, part of the bile duct, and sometimes part of the stomach. The remaining digestive tract is then reconstructed by connecting the pancreatic remnant, bile duct, and stomach to the small intestine. It is one of the most complex abdominal operations in oncology, requiring an experienced surgical oncology team and dedicated post-operative critical care support.
What is the survival rate for pancreatic cancer in India?
Survival rates are strongly stage-dependent. Resected Stage I disease: five-year survival of approximately 20–30% following surgery and adjuvant chemotherapy. Borderline resectable disease that responds to neoadjuvant therapy and undergoes complete resection: similar or slightly lower. Locally advanced (Stage III) disease on chemotherapy: median survival of 12–15 months with current regimens. Metastatic (Stage IV) disease: median survival of 8–12 months with current combination chemotherapy. These figures reflect the natural aggressiveness of PDAC — but they are averages, and individual patients can and do exceed them, particularly with access to current NCCN-protocol care at a specialist centre.
Can pancreatic cancer be treated without surgery?
Yes. For the majority of patients — approximately 80% who present with locally advanced or metastatic disease — chemotherapy, chemoradiation, and palliative supportive care are the primary treatments. Chemotherapy for advanced pancreatic cancer uses gemcitabine + nab-paclitaxel or FOLFIRINOX regimens that improve survival and quality of life compared to no treatment. Chemoradiation controls local disease progression in Stage III. Biliary stenting relieves jaundice without surgery. Coeliac plexus neurolysis provides pain relief without abdominal surgery. For patients with BRCA-mutated disease responding to platinum chemotherapy, olaparib maintenance therapy is an oral targeted option requiring no surgical intervention.
What is the difference between resectable and non-resectable pancreatic cancer?
Resectable pancreatic cancer is confined to the pancreas with clear planes around all major blood vessels — it can be completely removed with surgery. Borderline resectable cancer abuts (touches) major vessels like the superior mesenteric artery, portal vein, or coeliac axis without fully encasing them — it may become resectable after neoadjuvant chemotherapy. Locally advanced (unresectable) cancer encases or involves major vessels and cannot be safely removed even after chemotherapy. Metastatic cancer has spread to distant organs (liver, lungs, peritoneum) and surgery is not part of the treatment plan. The distinction between resectable and borderline resectable — which requires specialist radiological and surgical review of high-quality CT — is the most important clinical decision in pancreatic cancer management.
What is a pancreatic neuroendocrine tumour (PNET)?
A PNET is a tumour arising from the hormone-producing islet cells of the pancreas — completely different from pancreatic adenocarcinoma in biology, behaviour, and treatment. PNETs are generally slower-growing and more amenable to surgery, with significantly better prognosis than PDAC. They are classified as functioning (producing hormones like insulin, glucagon, or gastrin causing specific symptoms) or non-functioning (causing no hormone syndrome, often discovered incidentally). Localised PNETs are treated with surgery. Advanced PNETs are managed with somatostatin analogues (octreotide, lanreotide), everolimus, sunitinib, or PRRT depending on grade and extent of disease. If you have been diagnosed with a PNET, ensure you are being managed by an oncologist experienced with neuroendocrine tumours specifically.
Can I get a second opinion before pancreatic cancer surgery?
Absolutely — and for pancreatic cancer, it is strongly advisable. The Whipple procedure is one of the most complex abdominal operations in oncology; the resectability decision is nuanced and requires specialist CT review and surgical judgement; and the choice between upfront surgery and neoadjuvant chemotherapy first for borderline resectable disease significantly affects outcomes. CION offers a dedicated Second Opinion service where our multidisciplinary tumour board reviews your imaging, pathology, and existing treatment recommendation before advising on the most appropriate course of action. If you have been told your cancer is 'inoperable' or 'borderline,' a second opinion may open options you have not yet been offered.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.