Rectal Cancer · Hyderabad's Dedicated Colorectal Team
Rectal Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Rectal cancer is one of the most treatable gastrointestinal cancers — but only when managed by a team that treats it as its own disease, not as an afterthought within a generic colorectal protocol. At CION, our colorectal oncology team delivers the full spectrum of rectal cancer care — from neoadjuvant chemoradiation and sphincter-preserving TME surgery to Watch-and-Wait for selected complete responders — across 7 Hyderabad locations, backed by NABH accreditation and NCCN-protocol care.
TME-based surgery — gold-standard technique reducing local recurrence from ~40% to <4%
Watch-and-Wait pathway — 15–30% of patients may avoid surgery entirely after a complete response
Sphincter preservation maximised — LAR vs APR decision reviewed at tumour board
Molecular testing (RAS/BRAF/MSI-H) — standard workup so the right targeted drug is chosen from diagnosis
4.8 · 800+ Google reviews · 15,000+ patients treated
17+
Cancer Specialists on Panel
96.9%
Breast Cancer Survival Rate*
15,000+
Patients Treated
4.8★
Google Rating (800+ reviews)
Written by Dr. Vajja Sandeep Kumar
Surgical Oncologist · MBBS · MS Surgical Oncology · DrNB Surgical Oncology · CION Cancer Clinics, Hyderabad
Medically reviewed by Dr. Bharati Devi Gorantla — Medical Oncologist · ECMO (European Certified Medical Oncologist, 2023) · MRCP SCE (UK) Medical Oncology (2024). Last reviewed: 20 May 2026.
The Critical Difference
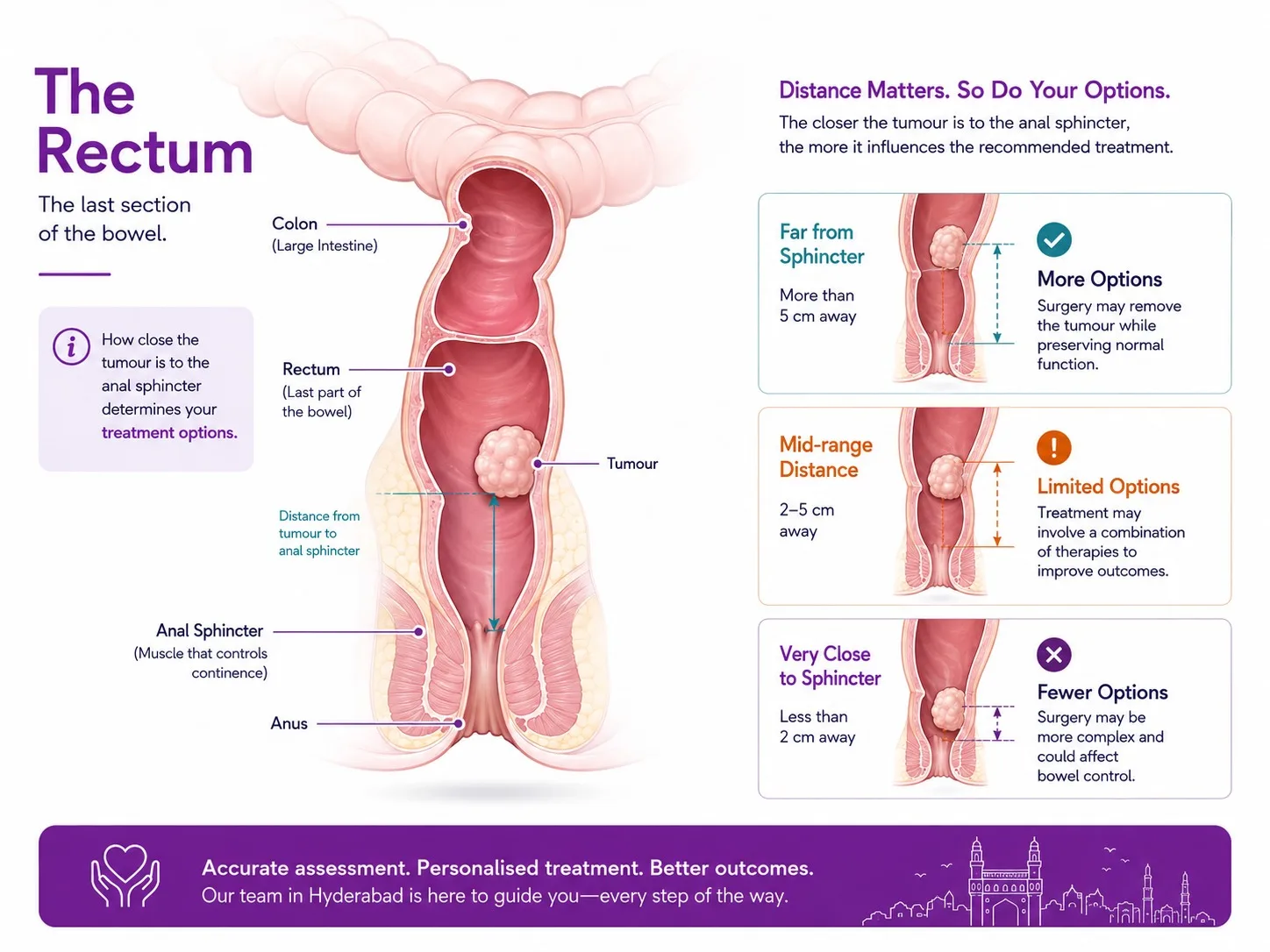
Rectal Cancer vs Colon Cancer — Why the Difference Matters
How close the tumour sits to the anal sphincter is the single biggest factor in whether natural bowel control can be preserved.
Rectal cancer and colon cancer are often grouped together as 'colorectal cancer' — and they do share risk factors, symptoms, and some treatments. But rectal cancer has a distinct treatment pathway that is quite different from colon cancer, and the two should not be managed the same way (watch a Mayo Clinic doctor explain how colon and rectal cancers are treated differently).
The rectum is the final 12–15cm of the large intestine, just above the anus. Its location deep in the pelvis — close to the bladder, urinary tract, reproductive organs, and the nerve and muscle structures that control bowel control — makes surgery more complex. The confined space means the cancer is harder to remove with clear margins. And radiation therapy, which plays a small role in colon cancer, is a central part of standard rectal cancer treatment.
The key practical differences for patients
Rectal cancer usually requires chemotherapy and radiation BEFORE surgery — not after; this is standard for most Stage II and Stage III cases and is not the approach for colon cancer.
The surgical technique — Total Mesorectal Excision (TME) — is specific to rectal cancer surgery and significantly affects whether the cancer comes back.
Some rectal cancer patients can avoid surgery entirely after treatment, with close monitoring instead — an option that does not exist for colon cancer.
A permanent colostomy bag is sometimes required — though far less often than patients fear, and this decision depends heavily on the tumour's location and response to treatment.
If you have been diagnosed with rectal cancer, make sure you are being managed by a team that treats rectal cancer as its own disease — not as an afterthought within a general colorectal protocol.
Did You Know?
India reported approximately 37,000 new rectal cancer cases in 2020, with numbers expected to rise to over 41,500 by 2025 according to ICMR data. Rectal cancer is among the most common gastrointestinal cancers in both men and women in urban India — driven by rising rates of processed food consumption, sedentary lifestyles, and obesity in cities like Hyderabad.
Risk Factors
What Increases the Risk of Rectal Cancer?
Diet high in red meat (beef, lamb, pork) and processed meats (sausages, bacon) — consistently associated with colorectal cancer risk.
Low-fibre diet — insufficient fruit, vegetables, and whole grains increases transit time in the bowel.
Inflammatory bowel disease — Crohn's disease and ulcerative colitis significantly elevate colorectal cancer risk over time.
Family history — first-degree relatives with colorectal cancer double your risk.
Lynch syndrome (HNPCC) and Familial Adenomatous Polyposis (FAP) — inherited conditions causing high lifetime colorectal cancer risk; genetic testing and early screening are strongly recommended for affected families.
Age above 50 — risk increases substantially after 50; colonoscopy screening is recommended from this age.
Obesity, sedentary lifestyle, smoking, and heavy alcohol use — all independently associated with increased risk.
If you have a family member diagnosed with colorectal cancer — particularly before the age of 60 — speak to a CION oncologist about genetic testing for Lynch syndrome. Identifying this hereditary condition can guide screening for you and other family members before cancer develops.
Symptoms
Symptoms of Rectal Cancer
Rectal cancer often causes symptoms that are easy to attribute to more common conditions like haemorrhoids or irritable bowel syndrome. The key is persistence — symptoms that do not resolve after a few weeks should prompt specialist evaluation and colonoscopy.
Rectal bleeding or blood in the stool — the most common presenting symptom; never assume this is haemorrhoids without investigation.
A change in bowel habits lasting more than 2–4 weeks — persistent diarrhoea, constipation, or stools that are narrower than usual.
Tenesmus — a feeling that the bowel has not fully emptied after passing a motion, even when it has.
Abdominal cramping, bloating, gas, or discomfort.
Unexplained weight loss and persistent fatigue.
Anaemia (low blood count) without an obvious cause — often from slow occult bleeding from a tumour.
Rectal bleeding is never normal. Even if you have haemorrhoids, any new rectal bleeding in a person over 40 should be investigated with at minimum a digital rectal examination and ideally a colonoscopy.
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the Specialists
Senior colorectal oncology specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Speak to a Rectal Cancer Specialist Today
Whether you've just received a diagnosis, want to know if Watch-and-Wait is an option, or need a second opinion before surgery — same-week appointments across 7 Hyderabad locations.
Accurate diagnosis and staging is the foundation of the right treatment plan. For rectal cancer, staging is more complex than for colon cancer — pelvic MRI is essential to guide decisions about surgery.
Colonoscopy and Biopsy
Colonoscopy directly visualises the rectal tumour and obtains a tissue biopsy for histopathological diagnosis. It also examines the entire colon for synchronous polyps or lesions. Flexible sigmoidoscopy is an alternative for lower rectal tumours. Biopsy tissue is also used for molecular testing — RAS status, BRAF V600E, and MSI-H/dMMR — which directly determines which systemic drugs are appropriate.
Pelvic MRI — The Most Important Staging Investigation for Rectal Cancer
High-quality pelvic MRI is the gold standard for rectal cancer staging. It tells the surgeon exactly how deeply the cancer has grown into the rectal wall (T stage), whether it has spread to nearby lymph nodes (N stage), and critically — whether there is a clear plane of tissue between the tumour and the circular 'envelope' of tissue surrounding the rectum (called the circumferential resection margin or CRM). If the cancer is close to this margin on MRI, neoadjuvant chemoradiation is used to shrink it before surgery. Pelvic MRI is performed before treatment and again after neoadjuvant chemoradiation to assess response.
Additional Staging
CT Scan (chest, abdomen, pelvis) — assesses spread to the liver, lungs, and distant lymph nodes.
PET-CT — for equivocal findings on CT or suspected recurrence.
Endoscopic Ultrasound (EUS) — for very early T1 tumours being considered for local excision without full TME.
Carcinoembryonic Antigen (CEA) blood test — a tumour marker used for baseline, treatment monitoring, and surveillance.
Staging & Outlook
Rectal Cancer Staging and Survival Rates
Rectal cancer staging uses the AJCC TNM system. Pelvic MRI provides the most accurate pre-treatment staging. The mrT stage (MRI-based T stage) is the key staging tool used by CION's multidisciplinary team to plan neoadjuvant treatment.
Stage
What it means
Typical plan
5-yr outlook (NCCN-grade care)
Stage I
Tumour into rectal wall (T1–T2) only · No nodes, no spread
Surgery (TME) alone; local excision for select T1
85–95%
Stage II
Through rectal wall (T3–T4) · No nodes, no spread
Neoadjuvant CCRT → TME → adjuvant chemotherapy
65–80%
Stage III
Any T with regional lymph nodes involved
Neoadjuvant CCRT → TME → adjuvant chemotherapy
45–65%
Stage IV
Any T, any N, with distant spread (liver, lungs, nodes)
Systemic chemotherapy ± targeted therapy; surgery for selected cases
15–30%
*5-year survival estimates are for rectal adenocarcinoma treated at specialist centres with TME surgery and modern systemic therapy. Individual outcomes depend on tumour biology, molecular profile, and completeness of treatment.
Step 1 — Treatment Before Surgery
Neoadjuvant Chemoradiation: Treatment Before Surgery
For most patients with Stage II or Stage III rectal cancer, the treatment journey begins not with surgery but with a course of chemotherapy and radiation together — given before the operation. This is called neoadjuvant chemoradiation (NACRT), and it is one of the most important advances in rectal cancer treatment of the past three decades.
Why it works and why it matters
It shrinks the tumour — making surgery easier, less extensive, and more likely to achieve clear margins.
It reduces local recurrence — the most common and most difficult type of recurrence to treat.
It increases sphincter preservation — fewer patients end up with a permanent colostomy bag.
15–30% achieve a complete response — the tumour shrinks so completely it cannot be found on MRI or endoscopy. These patients may be candidates for Watch-and-Wait rather than immediate surgery.
Standard neoadjuvant chemoradiation at CION involves 5–6 weeks of daily radiation to the pelvis with concurrent oral or intravenous chemotherapy (typically capecitabine or 5-fluorouracil). After treatment ends, patients rest for 8–12 weeks while the tumour continues to respond — then undergo MRI and endoscopy to assess the response before any surgical decision is made.
An important recent development: Total Neoadjuvant Treatment (TNT) — giving additional chemotherapy alongside the standard chemoradiation, all before surgery — is an emerging NCCN-supported approach that is showing even better tumour response rates and more patients achieving complete response. CION's tumour board discusses TNT for appropriate candidates.
Differentiator
Watch-and-Wait — Could You Avoid Surgery Altogether?
This is one of the most important questions in modern rectal cancer treatment — and one that few hospital treatment pages in Hyderabad currently address. The answer, for some patients, is yes.
After neoadjuvant chemoradiation, the tumour is reassessed with MRI and endoscopy. In roughly 15–30% of patients, the tumour has completely disappeared — there is no visible cancer on imaging or examination. These patients are said to have achieved a complete clinical response (cCR). For these patients, an approach called Watch-and-Wait has been established as a safe alternative to proceeding directly to surgery.
What Watch-and-Wait means
No surgery — at least initially.
Very close monitoring every 3 months with MRI pelvis, endoscopy, and CEA blood test for the first 2 years.
If the cancer stays gone, monitoring continues and surgery may never be needed.
If there are signs of regrowth, surgery is performed at that point — and outcomes remain excellent because the regrowth is detected early.
Multiple studies — including data from the Indian subcontinent — have shown that Watch-and-Wait achieves similar long-term survival to immediate surgery in complete responders, while preserving the rectum, avoiding surgical complications, and in many cases preventing a permanent colostomy bag. It is now endorsed by NCCN and ESMO for carefully selected patients.
Watch-and-Wait is not suitable for everyone — it requires strict patient selection, commitment to close follow-up, and an experienced multidisciplinary team to make the assessment. But if you have completed chemoradiation and have been told the cancer has responded well, it is a question worth asking before accepting surgery: "Has my response been assessed for Watch-and-Wait eligibility?"
Surgery
Surgery for Rectal Cancer — TME and the Colostomy Question
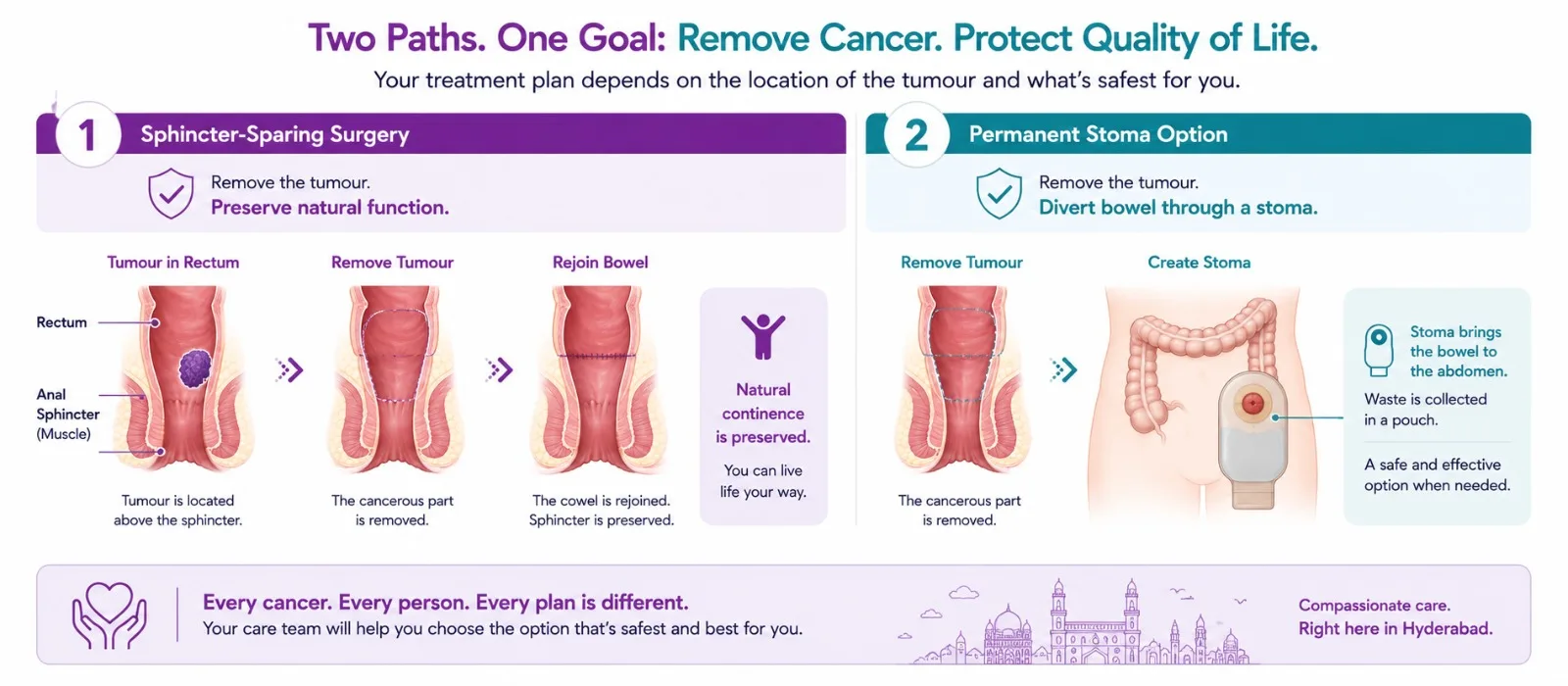
Wherever it is safe, sphincter-sparing surgery removes the cancer and rejoins the bowel — preserving natural continence.
When surgery is indicated — either as primary treatment for early-stage disease or after neoadjuvant chemoradiation — the surgical technique used determines whether the cancer comes back. This is where Total Mesorectal Excision (TME) matters.
What Is TME and Why Does It Matter?
The rectum is surrounded by a fatty tissue envelope called the mesorectum, which contains the blood vessels, lymph nodes, and lymphatic channels through which rectal cancer spreads locally. Total Mesorectal Excision means removing the rectum together with this entire mesorectal envelope — cutting precisely along the natural tissue plane that surrounds it, without cutting into the envelope itself.
When this plane is followed correctly, it leaves no cancer cells behind in the pelvis and reduces local recurrence rates from approximately 40% (with older surgical techniques) to less than 4% in specialist centres. When the plane is violated — cutting into the mesorectum rather than around it — cancer cells are left behind and local recurrence rates are dramatically higher.
TME is the gold standard for rectal cancer surgery everywhere in the world. It can be performed open (traditional), laparoscopically (keyhole), or robotically (robot-assisted keyhole). At CION, our surgical oncology team performs TME-based rectal cancer surgery, with the approach chosen based on tumour location, patient build, and prior treatment.
Will I Need a Colostomy Bag?
This is the question most patients and families ask first — and it deserves an honest, clear answer rather than a vague reassurance. There are two main types of rectal cancer surgery:
Low Anterior Resection (LAR) — the rectum is removed and the remaining colon is joined to the anal canal, preserving the ability to pass stools normally. This is sphincter-preserving surgery. Most patients with mid or upper rectal cancer who have a good response to neoadjuvant chemoradiation can have LAR. A temporary loop ileostomy is often created at the same time to protect the join while it heals — but this is reversed in a second operation 3–6 months later, and the patient returns to normal bowel function.
Abdominoperineal Resection (APR) — the rectum and the anal sphincter muscles are removed together, and a permanent end colostomy is created. APR is reserved for cancers in the very lowest part of the rectum that directly involve the sphincter muscles — and the decision to perform APR vs LAR is reassessed after neoadjuvant chemoradiation to see whether shrinkage has made sphincter preservation possible.
The bottom line: the majority of rectal cancer patients do not end up with a permanent colostomy bag. Neoadjuvant chemoradiation, careful surgical planning, and experienced TME surgery together maximise the chance of sphincter preservation. CION's tumour board makes this assessment for every patient before surgery is planned.
Medical Oncology
Systemic Therapy — Chemotherapy, Targeted Therapy, and Immunotherapy
Adjuvant Chemotherapy After Surgery
After surgery for Stage II or Stage III rectal cancer, most patients receive 6 months of adjuvant chemotherapy — typically FOLFOX (oxaliplatin + leucovorin + 5-fluorouracil) or CAPOX (capecitabine + oxaliplatin) — to mop up any cancer cells that may have spread beyond the rectum and reduce the risk of recurrence. CION's medical oncology team, led by Dr. Bharati Devi Gorantla (ECMO 2023, MRCP UK 2024), delivers these regimens in a comfortable day-care setting.
Systemic Therapy for Advanced (Stage IV) Rectal Cancer
For Stage IV rectal cancer — where the cancer has spread to the liver, lungs, or other organs — systemic chemotherapy combined with targeted therapy is the primary treatment. The choice of targeted drug depends on molecular testing of the tumour:
RAS mutation status (KRAS and NRAS) — if the tumour is RAS wild-type, anti-EGFR antibodies such as cetuximab (Erbitux) or panitumumab can be added to chemotherapy. If RAS mutated, anti-EGFR therapy does not work and bevacizumab is used instead.
BRAF V600E mutation — a BRAF-mutated rectal cancer has a distinct biology and may benefit from BRAF-targeted therapy combinations.
MSI-H / dMMR status — approximately 3–5% of colorectal cancers have a defect in the DNA mismatch repair system. These tumours respond dramatically to immune checkpoint inhibitors — pembrolizumab or nivolumab — which can achieve long-lasting responses that chemotherapy cannot. NCCN now recommends pembrolizumab as first-line treatment for MSI-H/dMMR metastatic colorectal cancer.
Bevacizumab — an anti-angiogenic antibody that cuts off the tumour's blood supply; used with chemotherapy for RAS-mutated or BRAF-mutated advanced colorectal cancer.
At CION, molecular testing (RAS, BRAF, MSI-H/dMMR) is performed on biopsy tissue for all advanced rectal cancer patients as standard workup — because these results directly determine the most effective treatment regimen for that specific patient.
Liver Metastases — When Surgery Is Possible
For selected patients with Stage IV rectal cancer where the spread is limited to the liver, surgical removal of liver metastases (hepatectomy) alongside treatment of the primary rectal tumour can achieve long-term cure in a meaningful proportion of patients. CION's multidisciplinary tumour board evaluates every Stage IV rectal cancer patient for resectability of liver metastases. Where liver surgery is recommended, CION coordinates with accredited hepatobiliary surgical centres for this component of care.
Quality of Life
Life After Rectal Cancer Surgery — LARS and Stoma Reversal
Two practical quality-of-life topics that few hospital treatment pages in Hyderabad currently address — but that every rectal cancer patient going into surgery deserves to know about.
Low Anterior Resection Syndrome (LARS)
After sphincter-preserving surgery for rectal cancer, many patients experience a cluster of bowel symptoms in the months following surgery — collectively called Low Anterior Resection Syndrome (LARS). These symptoms include: frequent bowel movements, urgency (needing to rush to the toilet), clustering (several bowel movements close together), incontinence, and difficulty emptying the bowel completely.
LARS occurs because the reservoir function of the rectum is lost after it is removed, and the nerve supply to the bowel can be affected by surgery and radiation. The severity ranges from mild to significant. The good news is that LARS typically improves over the first 1–2 years after surgery as the bowel adapts. CION's care team discusses LARS management with every surgical patient — including dietary adjustments, pelvic floor physiotherapy, and other supportive measures.
Stoma Reversal
Most patients who have a temporary ileostomy (loop stoma) after Low Anterior Resection have it reversed 3–6 months after surgery, once the bowel join has healed fully. Reversal is a planned second surgery — shorter and simpler than the original operation — after which normal bowel function is restored. CION plans stoma reversal as part of the overall surgical pathway for every appropriate patient from the outset, so patients know from day one that the stoma is temporary.
How Decisions Are Made
Multidisciplinary Tumour Board — Every Case Reviewed by a Team
Rectal cancer requires more complex multidisciplinary decision-making than almost any other gastrointestinal cancer. The treatment sequence — when to give chemoradiation, whether Watch-and-Wait is appropriate, which surgical approach to use, whether liver metastases are resectable — requires surgical oncology, medical oncology, radiation oncology, radiology, and pathology to work together from the start. At CION:
Pelvic MRI reviewed by specialist radiologists to determine mrT stage and circumferential resection margin status.
Neoadjuvant chemoradiation vs upfront surgery decision made at tumour board based on MRI staging.
Total Neoadjuvant Treatment (TNT) evaluated for appropriate candidates.
Post-chemoradiation response assessed — TME surgery or Watch-and-Wait decision.
LAR vs APR decision made based on tumour location, response to treatment, and patient preference — with sphincter preservation maximised wherever oncologically safe.
Molecular testing (RAS, BRAF, MSI-H/dMMR) arranged at diagnosis for all advanced cases.
Liver metastasis resectability evaluated at tumour board for Stage IV patients.
LARS management and stoma reversal planning built into the surgical pathway from the outset.
NCCN and ESMO Protocol Adherence across all stages — coordinated digitally across all 7 Hyderabad locations.
Why Patients Choose CION for Rectal Cancer Treatment in Hyderabad
Sixteen reasons our patients pick CION — rectal cancer treated as its own disease, TME surgery, Watch-and-Wait for eligible patients, and full quality-of-life planning.
1,000+ Rectal Cancer Cases
Treated every year across the CION network
7 locations across Hyderabad
Kukatpally, Kompally, Ameerpet, Tolichowki, MasabTank, L.B. Nagar, Banjara Hills — 70% less travel than single-centre hospitals
5-Star NABH Accredited
Cancer Care Institutes
NCCN & ESMO Protocol Adherence
Across all stages and subtypes
Rectal cancer as a distinct disease
Not an afterthought within a generic colorectal protocol
TME-based surgery
Gold standard technique reducing local recurrence from ~40% to <4%
Neoadjuvant chemoradiation for Stage II/III
Treatment before surgery to maximise outcomes
Watch-and-Wait pathway
For eligible complete responders — surgery avoided where evidence supports it
Sphincter preservation maximised
LAR vs APR decision reviewed at tumour board
Molecular testing (RAS/BRAF/MSI-H)
Standard workup — correct drug selected from diagnosis
European Certified Medical Oncologist
ECMO on the team for systemic therapy management
Lynch syndrome genetic testing
Offered to eligible families
LARS & stoma reversal planning
Built into the surgical pathway from day one
Dedicated Second Opinion service
Free written review of your MRI, pathology and existing plan
EMI facility
Flexible payment options for all patients
4.8 / 5 Google rating
Across 1,000+ patient reviews · 35+ centres across Telangana & AP
Transparent Costs
Rectal Cancer Treatment Cost in Hyderabad
Treatment costs vary depending on stage, whether neoadjuvant chemoradiation is required, the surgical approach, and systemic therapy needed. The following ranges are based on current Hyderabad market data:
Treatment
Approx. Cost (INR)
Notes
Neoadjuvant Chemoradiation (CCRT)
₹1,50,000 – ₹3,00,000
5–6 weeks radiation + concurrent chemotherapy
Low Anterior Resection (LAR) with TME
₹3,00,000 – ₹7,00,000
Laparoscopic at higher end; includes temporary stoma
Abdominoperineal Resection (APR)
₹3,50,000 – ₹8,00,000
Permanent colostomy; more extensive pelvic dissection
Stoma Reversal Surgery
₹1,00,000 – ₹2,50,000
Planned 3–6 months after LAR
Adjuvant Chemotherapy (per cycle)
₹25,000 – ₹80,000
FOLFOX / CAPOX; 12 cycles standard (6 months)
Targeted Therapy (per cycle)
₹60,000 – ₹1,80,000
Bevacizumab / cetuximab based on RAS testing
Immunotherapy — Pembrolizumab (per cycle)
₹1,00,000 – ₹2,50,000
For MSI-H/dMMR advanced rectal cancer
Full Multi-modal Treatment
₹3,00,000 – ₹15,00,000+
Depending on stage, surgical approach, and duration
Costs are indicative. A personalised cost estimate is provided following your initial oncology consultation at CION.
Financial Support Options
EMI Facility — flexible instalment-based payment options available for all patients.
Private Health Insurance — CION works with all major TPAs for cashless hospitalisation; targeted therapy and immunotherapy coverage varies by insurer.
Did You Know?
In 15–30% of rectal cancer patients who complete neoadjuvant chemoradiation, the cancer disappears completely on MRI and endoscopy. These patients may not need immediate surgery — the Watch-and-Wait approach, with close monitoring every 3 months, has been shown to achieve similar survival outcomes to immediate surgery while preserving the rectum and in many cases avoiding a colostomy bag. Ask your oncologist whether your response has been assessed for Watch-and-Wait eligibility.
Next Step
Book a 45-Minute Consultation — No Rushed Decisions
Bring your reports. Our oncologists will walk you through the staging, treatment options, expected costs, and quality-of-life impact — clearly and honestly.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
Rectal Cancer Treatment — Frequently Asked Questions
What is the best treatment for rectal cancer?
The best treatment depends on the stage. For Stage I rectal cancer, surgery with Total Mesorectal Excision (TME) — sphincter-preserving Low Anterior Resection (LAR) for most — is the primary treatment. For Stage II and III, the current standard is neoadjuvant chemoradiation (chemotherapy + radiation before surgery) followed by TME surgery and adjuvant chemotherapy. For Stage IV (spread to liver or lungs), systemic chemotherapy combined with targeted therapy — chosen based on molecular testing of the tumour — is the backbone, with surgery for selected patients whose spread is limited. In some patients who have a complete response to chemoradiation, Watch-and-Wait avoids surgery entirely. CION's multidisciplinary tumour board determines the right approach for every individual patient.
What is the cost of rectal cancer treatment in Hyderabad?
Treatment costs depend significantly on stage and approach. Neoadjuvant chemoradiation costs approximately ₹1,50,000 to ₹3,00,000. Low Anterior Resection (LAR) with TME costs ₹3,00,000 to ₹7,00,000. Adjuvant chemotherapy cycles (FOLFOX/CAPOX) cost ₹25,000 to ₹80,000 per cycle over 6 months. Targeted therapy (bevacizumab/cetuximab) costs ₹60,000 to ₹1,80,000 per cycle. Immunotherapy (pembrolizumab for MSI-H tumours) costs ₹1,00,000 to ₹2,50,000 per cycle. CION provides a personalised estimate after your initial consultation. EMI payment options are available.
Is rectal cancer curable?
Yes — rectal cancer is highly curable, particularly when detected at an early stage. Stage I has a 5-year survival rate of 85–95%. Stage II achieves 65–80% with neoadjuvant chemoradiation and TME surgery. Stage III has a 5-year survival of 45–65% with modern multimodal treatment. Stage IV rectal cancer is less often curable, but selected patients with liver-limited metastases can be cured with combined treatment — and even those with widespread Stage IV disease can live for several years on modern targeted therapy and immunotherapy regimens. Early detection through colonoscopy screening is the single most powerful tool for improving outcomes.
Will I need a colostomy bag for rectal cancer?
Not necessarily — and for most patients, not permanently. The need for a colostomy depends primarily on how low in the rectum the tumour is and whether neoadjuvant chemoradiation has shrunk it away from the sphincter muscles. Most patients with mid or upper rectal cancer can have sphincter-preserving surgery (Low Anterior Resection). Some patients have a temporary ileostomy to protect the surgical join while it heals — but this is reversed 3–6 months later. Only patients with cancers in the very lowest part of the rectum that directly involve the sphincter muscles require a permanent colostomy (APR). Even for these patients, neoadjuvant chemoradiation may shrink the tumour sufficiently to allow sphincter-sparing surgery — which is why reassessment after chemoradiation is so important before any surgical decision is finalised.
What is Total Mesorectal Excision (TME)?
TME is the gold standard surgical technique for rectal cancer — and the single most important determinant of whether the cancer comes back in the pelvis. The rectum is surrounded by a fatty tissue envelope called the mesorectum, which contains the blood vessels, lymph nodes, and lymphatic channels through which rectal cancer spreads locally. TME means removing the rectum together with this entire mesorectal envelope by cutting precisely along the natural tissue plane around it. When done correctly, it reduces local recurrence rates from approximately 40% (with older techniques) to less than 4%. When the plane is violated and cancer cells are left behind, recurrence rates are dramatically higher. This is why the surgical team performing your rectal cancer operation matters enormously.
What is the survival rate for rectal cancer in India?
5-year survival rates at specialist oncology centres: Stage I — 85–95%; Stage II — 65–80%; Stage III — 45–65%; Stage IV — 15–30% overall, though patients with resectable liver-limited metastases can achieve 30–50% 5-year survival with combined surgical and systemic treatment. India's overall colorectal cancer survival is lower than Western countries primarily because most patients present at Stage III or IV — reinforcing the importance of colonoscopy screening from age 50 (or earlier with family history) and prompt investigation of rectal bleeding or bowel changes.
What is neoadjuvant chemoradiation for rectal cancer?
Neoadjuvant chemoradiation (NACRT) means giving chemotherapy and radiation therapy together, before surgery — the opposite of the traditional approach where surgery came first. For Stage II and III rectal cancer, NACRT is now the standard of care rather than upfront surgery. It typically involves 5–6 weeks of daily radiation to the pelvis alongside oral or intravenous chemotherapy. After treatment, patients rest for 8–12 weeks while the tumour continues to respond. Then MRI and endoscopy assess the response before the surgery decision is made. NACRT shrinks the tumour, reduces the risk of local recurrence, increases the chance of sphincter-preserving surgery, and in 15–30% of patients achieves a complete response that allows Watch-and-Wait instead of surgery.
What is the difference between rectal cancer and colon cancer?
Both are colorectal cancers, but they have different treatment approaches. The key differences: Rectal cancer usually requires chemotherapy + radiation BEFORE surgery (neoadjuvant treatment) for Stage II/III disease; colon cancer typically has surgery first and chemotherapy after. Rectal cancer surgery uses a specific technique called TME that is not relevant to colon cancer surgery. Radiation therapy plays a central role in rectal cancer treatment but a minimal role in colon cancer. Some rectal cancer patients can avoid surgery entirely through Watch-and-Wait — this is not an option for colon cancer. The risk of needing a permanent colostomy is unique to rectal cancer (specifically low rectal tumours), not colon cancer.
Can rectal cancer come back after treatment?
Yes, rectal cancer can recur — which is why surveillance after treatment is essential. Local recurrence in the pelvis was historically common (up to 40%) but modern TME surgery combined with neoadjuvant chemoradiation has reduced this to less than 5–10% at specialist centres. Distant recurrence — most commonly in the liver or lungs — can occur even after successful primary treatment. Surveillance typically involves CEA blood tests every 3 months, CT scanning every 6 months, colonoscopy at 1 year post-surgery, and pelvic MRI where indicated. Patients in the Watch-and-Wait pathway have the most intensive monitoring — MRI + endoscopy + CEA every 3 months for the first 2 years. Most recurrences are detected during surveillance when treatment options are still available.
Can I get a second opinion before rectal cancer surgery?
Absolutely — and for rectal cancer, a second opinion is particularly valuable in several situations: if surgery has been recommended without prior neoadjuvant chemoradiation for a Stage II or III tumour; if a permanent colostomy has been recommended without reassessing after chemoradiation; if Watch-and-Wait has not been discussed despite a good treatment response; if molecular testing has not been arranged for advanced disease; and if the surgical team does not have specific experience with TME. CION offers a dedicated Second Opinion service where our multidisciplinary tumour board reviews your MRI, colonoscopy findings, pathology, and current treatment recommendation before advising on the best pathway forward.
Need a Second Opinion?
Free consultation with a specialist. No commitment.