
Hyderabad's Multidisciplinary Stomach Cancer Team
Stomach Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
Stomach cancer — also called gastric cancer — is one of the most commonly diagnosed gastrointestinal cancers in India, with a significantly higher incidence in South India including Telangana and Andhra Pradesh. At CION Cancer Clinics, our surgical and medical oncology team delivers the full spectrum of stomach cancer treatment — from endoscopic resection for early-stage disease and complex D2 gastrectomy to molecular-targeted therapy and first-line immunotherapy for advanced disease — across 7 Hyderabad locations, backed by NABH accreditation and NCCN protocol-driven care.
- NCCN & ESMO Protocol Adherence — across all stomach cancer subtypes and stages
- MCh Surgical Oncologist — D2 gastrectomy by Dr. Raghavendra Naik (MCh, SVIMS Tirupati)
- Perioperative Chemotherapy Pathway — FLOT regimen for resectable Stage II/III disease
- HER2 + PD-L1 Testing — trastuzumab for HER2+, nivolumab for CPS ≥5 advanced disease
17+
Cancer Specialists
on Panel
on Panel
96.9%
Breast Cancer
Survival Rate*
Survival Rate*
15,000+
Patients
Treated
Treated
4.8★
Google Rating
(800+ reviews)
(800+ reviews)
Stomach Cancer in Hyderabad — What You Need to Know
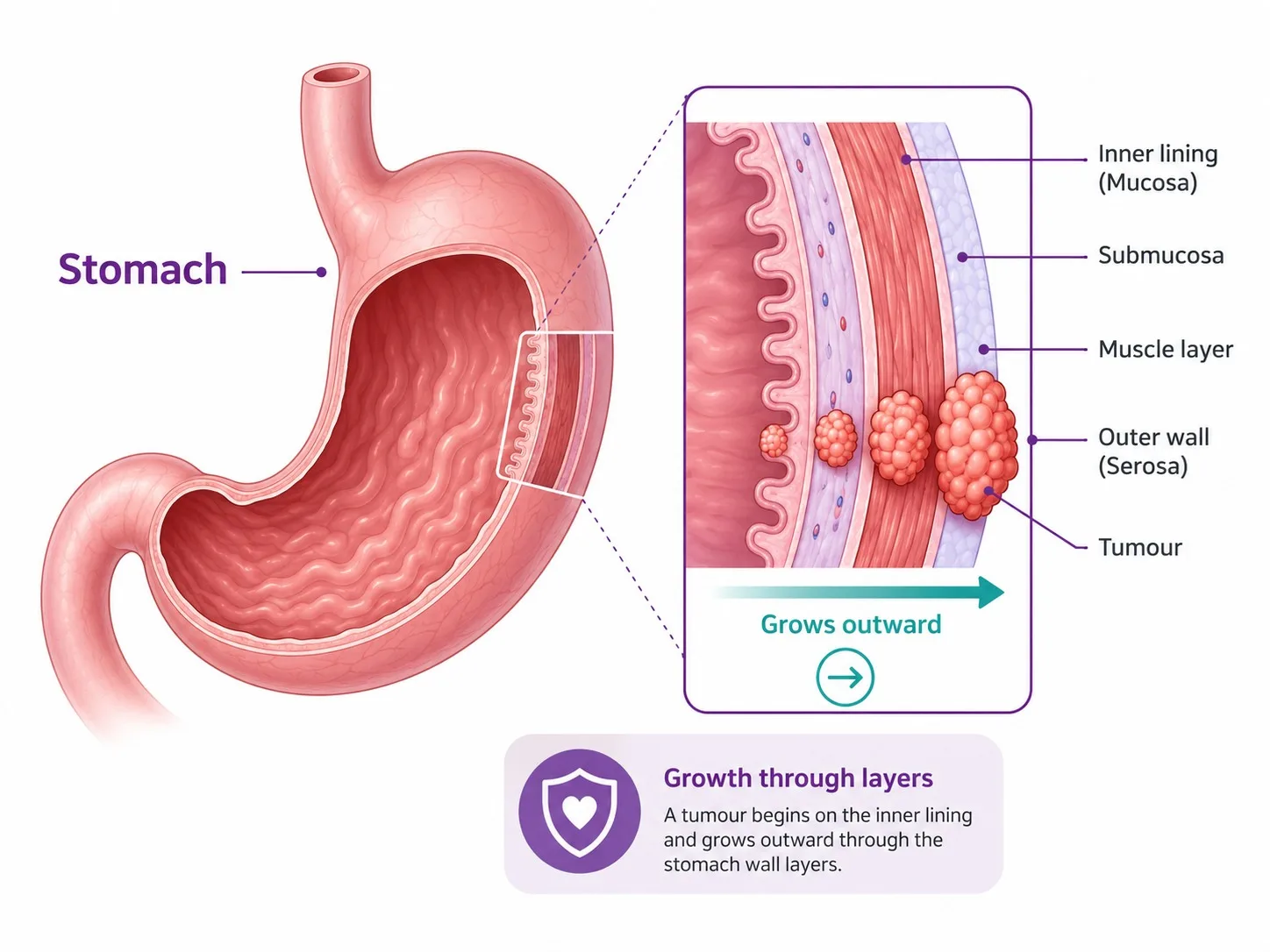
The stomach is a muscular organ in the upper abdomen that stores and digests food through gastric acid and enzymes. Stomach cancer develops when cells in the stomach lining acquire mutations and grow uncontrollably; for a plain-language overview you can watch a Mayo Clinic gastric cancer overview. In India, gastric cancer accounts for approximately 34,000 new cases annually, with a striking male-to-female ratio of 2:1. South India — including Telangana and Andhra Pradesh — has consistently higher gastric cancer rates than the national average, driven by a high prevalence of Helicobacter pylori (H. pylori) infection, dietary patterns including salted and pickled foods, and smoking.
Approximately 60–70% of stomach cancer patients in India are diagnosed at Stage III or Stage IV, when the disease has spread beyond the stomach. However, for the 30–40% diagnosed at an earlier, operable stage, modern treatment combining perioperative chemotherapy with surgery can achieve long-term cure or durable remission. Even at advanced stage, targeted therapy and immunotherapy have significantly extended survival compared to chemotherapy alone a decade ago.
Did You Know? India has one of the highest rates of Helicobacter pylori (H. pylori) infection globally — estimated at 50–80% of the adult population. H. pylori infection is the single most important preventable risk factor for gastric cancer. Testing and treating H. pylori in high-risk individuals can significantly reduce the risk of developing stomach cancer.
Types of Stomach Cancer We Treat
Stomach cancer is not one disease. The histological type — adenocarcinoma versus GIST versus lymphoma — determines the entire treatment pathway. CION's tumour board confirms the exact type before any treatment decision.
~95% of cases Gastric Adenocarcinoma
Arises from the glandular cells lining the stomach. Classified into two distinct subtypes with different behaviour and treatment implications:
- Intestinal-type — slow-growing; strongly associated with H. pylori, chronic gastritis, and dietary factors; more common in older men; generally more amenable to surgery
- Diffuse-type (incl. signet ring cell) — the more aggressive subtype; grows as individual cells infiltrating the stomach wall without forming a distinct mass; more common in younger patients and women; typically requires perioperative chemotherapy
Different pathway Gastrointestinal Stromal Tumour (GIST)
GIST is a completely different cancer from adenocarcinoma — it arises from the interstitial cells of Cajal in the stomach wall, not the lining. This distinction is critical because GISTs require an entirely different treatment approach: surgery for localised disease, and imatinib (a tyrosine kinase inhibitor) — not conventional chemotherapy — for advanced or metastatic GISTs. Standard gastric cancer chemotherapy regimens have no meaningful activity against GIST. CION's tumour board identifies and correctly pathways all GIST diagnoses.
Curable with antibiotics Gastric MALT Lymphoma
Mucosa-associated lymphoid tissue (MALT) lymphoma of the stomach is a low-grade B-cell lymphoma strongly associated with H. pylori infection. Remarkably, H. pylori eradication alone can induce complete remission in the majority of early-stage MALT lymphomas — making it one of the few cancers curable with antibiotics in early stages. Higher-grade gastric lymphomas are treated with standard lymphoma chemotherapy regimens (R-CHOP).
Neuroendocrine Carcinoid Tumours (Gastric NETs)
Gastric neuroendocrine tumours arise from the hormone-producing enterochromaffin-like cells of the stomach. Type I and Type II are low-grade and often managed with endoscopic resection and monitoring. Type III is sporadic, more aggressive, and treated with surgery similar to adenocarcinoma. CION manages gastric NETs through its neuroendocrine tumour pathway.
H. Pylori — The Most Important Preventable Risk Factor
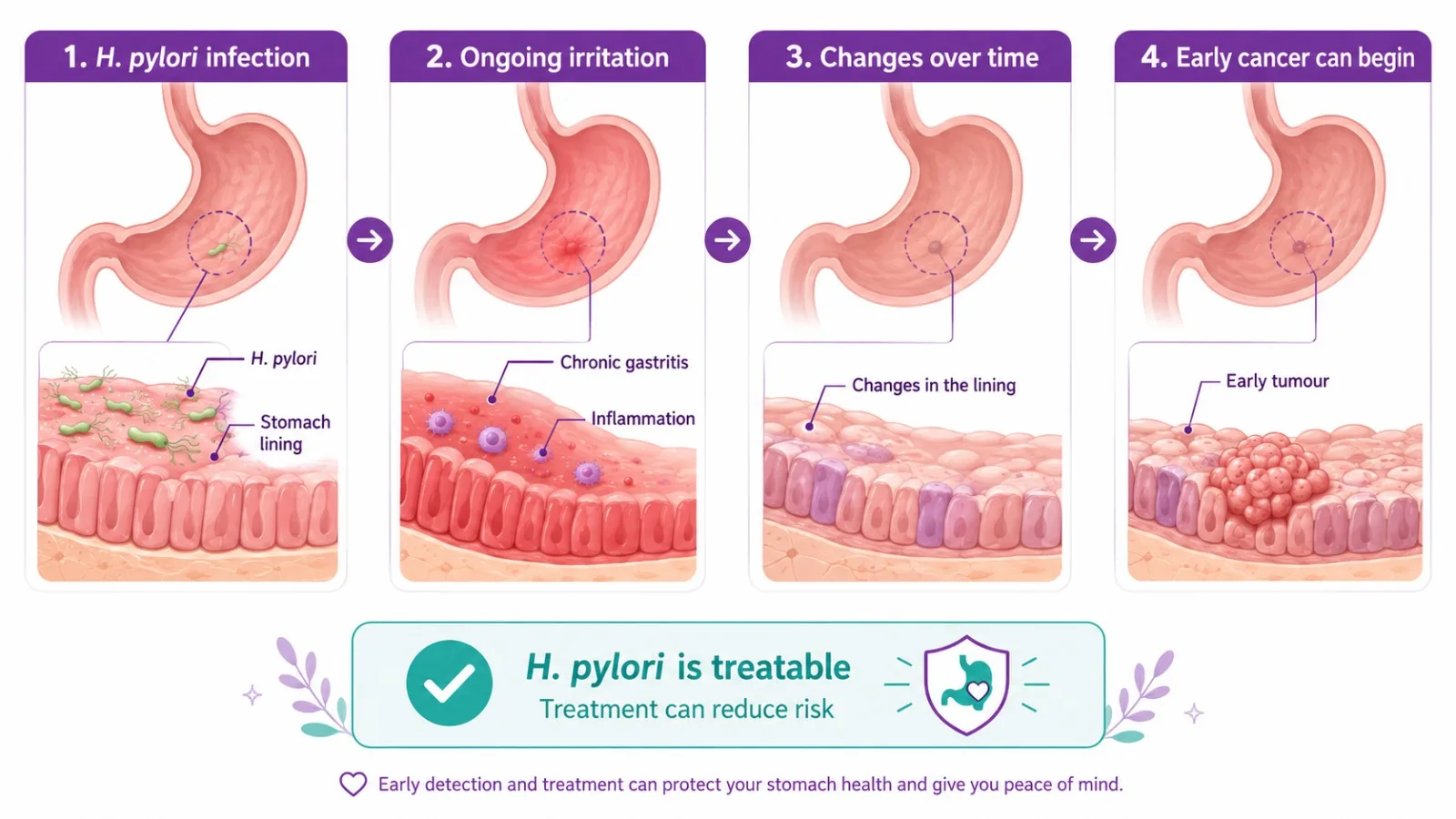
Helicobacter pylori is a spiral-shaped bacterium that infects the stomach lining, causing chronic inflammation (gastritis). Untreated chronic H. pylori gastritis progresses through a defined sequence — chronic gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → gastric cancer — over years to decades. H. pylori is classified as a Class I carcinogen by the WHO and is responsible for approximately 75–90% of all non-cardia gastric cancers.
In Hyderabad and across Telangana/AP, H. pylori prevalence is estimated at 60–70% — creating a significant population at elevated gastric cancer risk. CION recommends:
- H. pylori testing (urea breath test, stool antigen test, or endoscopic biopsy) for all patients with persistent dyspepsia, gastric ulcers, or a family history of stomach cancer
- H. pylori eradication therapy (standard triple or quadruple antibiotic regimens) for all confirmed H. pylori-positive individuals — this reduces gastric cancer risk and can cause regression of early MALT lymphoma
- Post-eradication confirmation testing to ensure successful treatment
If you have been diagnosed with H. pylori infection or have a family member with stomach cancer, speak to a CION oncologist about risk assessment and surveillance.
Other Risk Factors for Stomach Cancer
Beyond H. pylori, several factors increase the risk of developing stomach cancer. Discuss your personal risk profile with a CION specialist if more than one applies to you.
- Diet high in salted, smoked, pickled, and preserved foods — traditional preservation methods common in South Indian cuisine increase nitrite exposure
- Smoking and tobacco use — smokers have double the gastric cancer risk of non-smokers
- Family history of stomach cancer — first-degree relatives carry 2–3 times higher risk
- Hereditary Diffuse Gastric Cancer (HDGC) syndrome — CDH1 gene mutations; lifetime gastric cancer risk >80% in mutation carriers; prophylactic total gastrectomy considered
- Lynch syndrome — associated with intestinal-type gastric cancer
- Chronic atrophic gastritis, gastric polyps, and previous partial gastrectomy
- Age above 50 and male gender — gastric cancer is 2–3 times more common in men
- Obesity — increases risk for cardia (upper stomach) adenocarcinoma
Symptoms of Stomach Cancer
Stomach cancer is often called a 'silent' cancer — early-stage disease produces few or no symptoms, and the symptoms that do occur mimic common conditions like acid reflux, indigestion, or gastritis. This is why most patients are diagnosed at an advanced stage. Persistent symptoms beyond 2–4 weeks should prompt endoscopic evaluation, especially in patients over 40 or with risk factors.
- Persistent upper abdominal pain, discomfort, or burning — often confused with acid reflux or ulcers
- Early satiety — feeling full very quickly after starting a meal
- Unexplained and significant weight loss and loss of appetite
- Nausea and vomiting — vomiting of blood (haematemesis) is a red flag
- Difficulty swallowing (dysphagia) — for tumours at the gastro-oesophageal junction
- Black, tarry, or bloody stools — indicating bleeding from a gastric tumour
- Persistent bloating and indigestion not responding to medication
- Fatigue and anaemia from occult (hidden) bleeding
Any adult over 40 with new-onset dyspepsia, or persistent upper GI symptoms that do not resolve with standard treatment, should undergo upper GI endoscopy to exclude gastric cancer. Book a consultation with a stomach cancer specialist at your nearest CION location.
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.






Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centre
Beyond Hyderabad
35+ centres across Telangana & Andhra Pradesh
Travelling for treatment? We may have a centre right where you are.
Telangana
Andhra Pradesh
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.

Medical Oncologist

Medical Oncologist
Dr. C. Raghavendra Reddy
MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

Medical Oncologist
Dr. Bharati Devi Gorantla
MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

Medical Oncologist
Dr. Owais Mohammed
MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)

Medical Oncologist

Medical Oncologist

Surgical Oncologist
Dr. Muralidhar Muddusetty
MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)

Surgical Oncologist

Surgical Oncologist

Surgical Oncologist
Dr. Vinay Mamidala
MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)

Surgical Oncologist

Radiation Oncologist

Radiation Oncologist

Radiation Oncologist

Hematologist

Interventional Radiologist
Dr. Mohammed Imran

Surgical Oncologist
Dr. Vajja Sandeep Kumar
MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Surgical Oncologist
Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationBook an appointment with our specialist
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Take the next step with confidence
Meet our stomach cancer team across 7 Hyderabad locations. Same-week appointments. EMI options available.
Stomach Cancer Diagnosis at CION
An accurate diagnosis that establishes histological type, stage, and the molecular profile (HER2, PD-L1) is essential before any treatment decision. CION's diagnostic pathway integrates endoscopy, imaging, and molecular testing.
Upper GI Endoscopy — The Diagnostic Gold Standard
Upper gastrointestinal (GI) endoscopy is the only reliable method for directly visualising the stomach lining and obtaining tissue for biopsy. A thin flexible scope is passed through the mouth into the stomach while the patient is sedated. Any suspicious lesion is biopsied for histological confirmation. For early-stage lesions, chromoendoscopy and narrow-band imaging (NBI) can improve detection of subtle mucosal abnormalities.
HER2 Testing — Standard Workup for All Advanced Gastric Cancers
HER2 (Human Epidermal Growth Factor Receptor 2) overexpression occurs in approximately 15–20% of gastric adenocarcinomas. HER2 testing — by immunohistochemistry (IHC) and fluorescence in situ hybridisation (FISH) — is now recommended for all patients with advanced or metastatic gastric cancer, because HER2-positive status determines eligibility for trastuzumab therapy, which significantly improves survival. CION's pathology workflow includes HER2 testing as a standard part of advanced gastric cancer workup.
PD-L1 Testing for Immunotherapy Eligibility
PD-L1 combined positive score (CPS) testing is performed on tumour tissue to determine eligibility for nivolumab-based immunotherapy. Patients with CPS ≥5 derive the greatest benefit from nivolumab + chemotherapy as first-line treatment for advanced gastric cancer per the CheckMate-649 trial data.
Imaging and Staging
- CT Scan (chest, abdomen, pelvis) — standard staging investigation; assesses tumour size, regional lymph node involvement, and distant metastases
- PET-CT — for detecting distant metastases and assessing treatment response
- Endoscopic Ultrasound (EUS) — most accurate modality for T-staging (depth of tumour invasion into the stomach wall) and N-staging (regional lymph nodes); guides decisions about perioperative chemotherapy vs upfront surgery
- Staging laparoscopy — for patients with locally advanced disease; detects peritoneal metastases not visible on CT that would change the treatment plan
- CA 19-9 and CEA tumour markers — used alongside imaging for monitoring treatment response and surveillance
Stomach Cancer Staging and Survival Rates
Stomach cancer is staged using the TNM system. Stage at diagnosis is the primary determinant of treatment approach and outcome.
| Stage | TNM Status | Extent of Disease | 5-Year Survival | Primary Treatment |
|---|---|---|---|---|
| Stage I | T1–2, N0–1, M0 | Confined to stomach wall ± limited nodal involvement | 60–80% | ESD (T1a) or surgery ± adjuvant chemotherapy |
| Stage II | T1–3, N1–2, M0 | Deeper wall invasion or more nodal involvement | 40–60% | Perioperative chemotherapy + gastrectomy (D2) |
| Stage III | T2–4, N2–3, M0 | Extensive nodal involvement or adjacent organ invasion | 20–40% | Perioperative chemotherapy + gastrectomy; consider radiation |
| Stage IV | Any T, Any N, M1 | Distant metastases (liver, lungs, peritoneum) | 5–15% | Systemic chemotherapy ± trastuzumab (HER2+) ± nivolumab; palliative care |
5-year survival estimates reflect outcomes in specialist oncology settings. Individual outcomes depend on tumour histology, HER2 status, PD-L1 CPS, and extent of surgical resection.
Stomach Cancer Surgery at CION — Gastrectomy & D2 Lymphadenectomy
Surgery remains the only potentially curative treatment for resectable gastric cancer. CION's surgical oncology team, led by Dr. Raghavendra Naik (MCh Surgical Oncology, SVIMS Tirupati), performs gastrectomy with systematic D2 lymphadenectomy — the internationally recommended extent of lymph node dissection for curative gastric cancer surgery.
- Endoscopic Submucosal Dissection (ESD) — for Stage 0 and Stage IA (T1a) disease confined to the mucosa; achieves curative resection without open surgery, preserving the entire stomach; preferred for well-differentiated T1a tumours ≤2cm
- Subtotal / Partial Gastrectomy — removal of the distal portion (body and antrum) with D2 lymphadenectomy and reconstruction; preferred for distal (antrum/pylorus) tumours when adequate proximal margins can be achieved; preserves a portion of the stomach for better nutritional outcomes
- Total Gastrectomy — removal of the entire stomach with D2 lymphadenectomy and oesophagojejunal anastomosis (Roux-en-Y reconstruction); required for proximal tumours, fundal tumours, and diffuse-type gastric cancer involving most of the stomach; requires lifelong nutritional supplementation including B12 injections
- D2 Lymphadenectomy — systematic dissection of perigastric and regional lymph node stations; NCCN/ESMO standard; provides accurate pathological staging and improves cure rates compared to more limited (D1) dissection
- Laparoscopic Gastrectomy — minimally invasive approach for T1 and selected T2 tumours; equivalent oncological outcomes to open surgery with significantly less blood loss, shorter hospital stay, and faster recovery
- HIPEC (Hyperthermic Intraperitoneal Chemotherapy) — heated chemotherapy delivered directly into the peritoneal cavity during surgery for selected patients with limited peritoneal metastases or as a prophylactic measure in high-risk cases
Perioperative Chemotherapy — The Standard of Care No Hospital Page in Hyderabad Explains
For patients with Stage II and Stage III resectable gastric cancer, surgery alone is no longer the recommended approach. Perioperative chemotherapy — giving chemotherapy before surgery to shrink the tumour, treat micrometastases, and improve the chance of complete resection, then completing chemotherapy after surgery — is the current NCCN and ESMO standard of care. It has been shown to significantly improve overall survival and R0 resection rates compared to surgery alone.
No hospital treatment page in Hyderabad currently explains this concept. CION's perioperative chemotherapy pathway for resectable Stage II/III gastric cancer:
-
1
Pre-treatment staging
Confirm resectability with EUS, CT, and staging laparoscopy where indicated; HER2 and PD-L1 testing performed on biopsy tissue.
-
2
Neoadjuvant chemotherapy
3 cycles of FLOT (docetaxel + oxaliplatin + leucovorin + 5-fluorouracil) or XELOX (capecitabine + oxaliplatin) before surgery; FLOT is the ESMO preferred regimen based on superior pathological response rates.
-
3
Re-staging
CT scan after neoadjuvant chemotherapy to assess tumour response and confirm resectability.
-
4
Surgery
Gastrectomy with D2 lymphadenectomy, targeting R0 resection.
-
5
Adjuvant chemotherapy
3 further cycles of the same regimen post-surgery to eliminate residual microscopic disease.
If you have been diagnosed with Stage II or Stage III stomach cancer and have only been offered surgery without pre-operative chemotherapy — or if you have not had staging laparoscopy to confirm the absence of peritoneal disease — request a second opinion from CION's tumour board before proceeding.
Targeted Therapy and Immunotherapy for Advanced Gastric Cancer
The appropriate first-line regimen for advanced gastric cancer now depends on the tumour's molecular profile — specifically HER2 status and PD-L1 CPS — making molecular testing at diagnosis essential. These protocols are entirely absent from most competitor hospital pages in Hyderabad.
15–20% of cases
HER2-Positive — Trastuzumab
For patients whose tumours overexpress HER2, trastuzumab (Herceptin) combined with platinum-based chemotherapy (cisplatin + capecitabine or 5-fluorouracil) is the NCCN Category 1 first-line treatment for advanced HER2-positive gastric cancer. The landmark ToGA trial demonstrated improved median overall survival of 13.8 months versus 11.1 months with chemotherapy alone. HER2 testing by IHC/FISH is performed before first-line treatment is selected.
PD-L1 CPS ≥5
HER2-Negative — Nivolumab + Chemotherapy
For HER2-negative advanced gastric cancer with PD-L1 CPS ≥5, nivolumab (an immune checkpoint inhibitor) with platinum-based chemotherapy is NCCN Category 1 first-line treatment. The CheckMate-649 trial demonstrated improved median overall survival of 14.4 months versus 11.1 months with chemotherapy alone in the CPS ≥5 population. CION performs PD-L1 CPS testing on all advanced gastric cancer biopsies.
Second-line
Second-Line and Subsequent Therapy
Ramucirumab (anti-VEGFR2) ± paclitaxel — NCCN second-line treatment; restricts tumour angiogenesis. Irinotecan monotherapy — alternative second-line option. Trastuzumab deruxtecan (T-DXd) — for HER2-positive disease that progressed after first-line trastuzumab. Pembrolizumab — for MSI-H/dMMR tumours at any line, and TMB-high tumours.
Not chemotherapy
GIST — Imatinib, Not Chemotherapy
Gastrointestinal stromal tumours (GISTs) require completely different systemic treatment from adenocarcinoma. Surgery is the definitive treatment for resectable GISTs. For unresectable or metastatic GISTs, imatinib (a tyrosine kinase inhibitor targeting the KIT or PDGFRA mutation driving most GISTs) is the first-line treatment — not conventional cytotoxic chemotherapy. Sunitinib is used for imatinib-resistant disease; regorafenib as third-line.
Radiation Therapy for Stomach Cancer
CION's radiation oncology team uses advanced, precisely targeted techniques for selected stomach cancer indications:
- Chemoradiation (concurrent chemotherapy + radiation) — for unresectable locally advanced gastric cancer and gastro-oesophageal junction tumours; also used as adjuvant therapy for selected patients with positive surgical margins or insufficient lymph node dissection
- Palliative radiation — for pain control, bleeding management, or obstruction relief in advanced disease
- IMRT and IGRT — used to precisely target gastric tumours while protecting adjacent organs (kidneys, liver, spinal cord)
Post-Surgery Nutritional Rehabilitation — Critical for Recovery
Total gastrectomy removes the entire stomach, fundamentally changing the way the body digests and absorbs food. Partial gastrectomy has similar but less severe effects. Post-gastrectomy nutritional management is as important as the surgery itself — and is a patient concern no other hospital treatment page in Hyderabad adequately addresses.
- Dumping syndrome — rapid transit of food from the oesophagus directly to the small intestine; managed with small, frequent low-carbohydrate meals; eating slowly and avoiding liquids during meals
- Vitamin B12 deficiency — the stomach produces intrinsic factor required for B12 absorption; after total gastrectomy, lifelong B12 injections (not oral supplements) are essential to prevent neurological complications
- Iron deficiency — reduced gastric acid impairs iron absorption; regular monitoring and supplementation required
- Calcium and Vitamin D — reduced absorption increases bone loss risk; long-term supplementation recommended
- Pancreatic enzyme supplements — if pancreatic juice secretion is affected by reconstruction
- Structured nutrition plan — a dietitian-led plan is provided for all gastrectomy patients at CION; high-calorie, protein-rich, easy-to-digest meals gradually increased in volume
CION's integrated care team includes dedicated nutrition counsellors who work with gastrectomy patients from the pre-operative planning stage through the full post-operative recovery period.
Multidisciplinary Tumour Board — Every Case Reviewed by a Team
Stomach cancer management requires precise coordination between surgical oncology, medical oncology, radiation oncology, gastroenterology, pathology, and nutrition. At CION, every gastric cancer case is reviewed by our multidisciplinary tumour board before treatment:
- H. pylori status confirmed and eradication therapy initiated where appropriate
- HER2 and PD-L1 testing arranged at diagnosis for all advanced cases
- EUS-based T and N staging for resectability assessment
- Staging laparoscopy discussed for locally advanced cases to exclude peritoneal disease
- Perioperative chemotherapy vs upfront surgery decision for Stage II/III disease
- GIST vs adenocarcinoma pathway differentiation based on histology and IHC
- MALT lymphoma — H. pylori eradication as first-line treatment
- Nutritional rehabilitation plan established pre-operatively for gastrectomy patients
- Alignment with current NCCN and ESMO evidence-based guidelines
- Digital coordination across all 7 Hyderabad locations
Did You Know? The CheckMate-649 trial established nivolumab + chemotherapy as the new standard of care for first-line advanced HER2-negative gastric cancer with PD-L1 CPS ≥5, improving median overall survival from 11.1 to 14.4 months. Testing for both HER2 and PD-L1 CPS at diagnosis is now essential to select the correct first-line regimen.
Why Patients Choose CION for Stomach Cancer Treatment in Hyderabad
Eighteen reasons our patients pick CION — across volume, protocols, surgical expertise, molecular testing, and supportive care.
15,000+ patients treated
7 locations across Hyderabad
NABH Accredited
NCCN & ESMO Protocol Adherence
MCh-trained surgical oncologist
Perioperative chemotherapy pathway
HER2 testing as standard workup
PD-L1 CPS testing & nivolumab immunotherapy
GIST correctly pathwayed with imatinib
MALT lymphoma managed with H. pylori eradication
ESD for early-stage T1a disease
HIPEC coordinated
Post-gastrectomy nutritional rehabilitation
Multidisciplinary tumour board review
Dedicated Second Opinion service
EMI facility
4.8 / 5 Google rating
35+ centres across Telangana & AP
Stomach Cancer Treatment Cost in Hyderabad
Treatment costs vary significantly by stage and treatment approach. The following ranges are based on current Hyderabad market data:
| Treatment | Approx. Cost (INR) | Notes |
|---|---|---|
| Endoscopic Resection (ESD/EMR) | ₹50,000 – ₹1,50,000 | For early-stage T1a disease; day procedure |
| Subtotal / Partial Gastrectomy (Laparoscopic) | ₹2,50,000 – ₹5,00,000 | Shorter hospital stay vs open surgery |
| Total Gastrectomy (Open) | ₹3,00,000 – ₹7,00,000 | Complex reconstruction; ICU stay included |
| Chemotherapy (per cycle) | ₹30,000 – ₹1,20,000 | FLOT / XELOX regimens; 6 cycles standard |
| Trastuzumab (per cycle — HER2+) | ₹80,000 – ₹2,00,000 | Combined with platinum chemotherapy; may be covered under insurance |
| Nivolumab + Chemotherapy (per cycle) | ₹1,00,000 – ₹2,50,000 | For PD-L1 CPS ≥5 advanced disease |
| Radiation Therapy (full course) | ₹1,00,000 – ₹2,50,000 | IMRT/IGRT; chemoradiation at higher end |
| Full Multi-modal Treatment | ₹2,50,000 – ₹10,00,000+ | Depending on stage, histology, and treatment duration |
Costs are indicative. A personalised treatment cost estimate is provided following your initial oncology consultation at CION.
Financial Support Options
- EMI Facility — flexible instalment-based payment options available for all patients.
- Private Health Insurance — CION works with all major TPAs for cashless hospitalisation; trastuzumab and immunotherapy may be partially covered depending on your insurer.
Stomach Cancer Care Near You — In Hyderabad & Beyond
CION operates 35+ centres across Telangana and Andhra Pradesh. Find your nearest stomach cancer specialist or explore care options in your city.
Stomach Cancer Care in Hyderabad — by Location
Stomach Cancer Care Beyond Hyderabad
Travelling for treatment? We may have a centre right where you are — across Telangana and Andhra Pradesh.
Vizag
Warangal
Karimnagar
Nizamabad
Mahabubnagar
Suryapet
Nalgonda
Sangareddy
Siddipet
Vizianagaram
Srikakulam
Bobbili
Not seeing your city? Call 18002028726 — we'll connect you to the nearest CION centre or arrange a teleconsultation.
Real patient outcomes
Hear from patients who've completed treatment at CION
Diagnoses, treatment journeys, and outcomes — in our patients' own words.
Real Stories. Real Voices.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
























Read all 800+ reviews on Google
Start Your Story. Book Free Consultation.Frequently Asked Questions — Stomach Cancer Treatment
Common questions about stomach cancer treatment in Hyderabad — answered by CION's oncology team.
What are the symptoms of stomach cancer?
Stomach cancer symptoms are often subtle in early stages and easily mistaken for common digestive conditions. The most important signs to watch for include: persistent upper abdominal pain or discomfort not responding to antacids; early satiety — feeling full very quickly; unexplained significant weight loss and appetite loss; persistent nausea or vomiting, especially vomiting of blood; black or tarry stools indicating internal bleeding; and difficulty swallowing for tumours near the gastro-oesophageal junction. Any adult over 40 with new or persistent upper GI symptoms, or any patient with a known H. pylori infection, family history of stomach cancer, or chronic gastritis, should undergo endoscopy without delay.
What is the cost of stomach cancer treatment in Hyderabad?
Stomach cancer treatment costs in Hyderabad vary by stage and treatment approach. Endoscopic resection for early-stage disease costs approximately ₹50,000 to ₹1,50,000. Laparoscopic gastrectomy ranges from ₹2,50,000 to ₹5,00,000. Total gastrectomy (open) costs ₹3,00,000 to ₹7,00,000. Chemotherapy cycles range from ₹30,000 to ₹1,20,000 per cycle. Trastuzumab for HER2-positive disease costs ₹80,000 to ₹2,00,000 per cycle and may be partially covered by health insurance. CION provides a personalised estimate after your initial oncology consultation. EMI payment options are available.
Is stomach cancer curable?
Yes — stomach cancer is curable when detected early. Stage I and Stage II gastric cancer has 5-year survival rates of 60–80% and 40–60% respectively with surgery and perioperative chemotherapy. Even Stage III disease, when treated with the full perioperative protocol (neoadjuvant chemotherapy + D2 gastrectomy + adjuvant chemotherapy), achieves meaningful long-term survival in a proportion of patients. Stage IV disease is rarely curable but has seen meaningfully improved survival with targeted therapy (trastuzumab for HER2+ disease) and immunotherapy (nivolumab). Early detection through H. pylori testing, endoscopic surveillance in high-risk individuals, and prompt evaluation of symptoms remains the most powerful tool for improving outcomes.
What is gastrectomy surgery?
Gastrectomy is the surgical removal of part or all of the stomach. Subtotal (partial) gastrectomy removes the lower portion of the stomach containing the tumour plus a margin, preserving the upper stomach; it is used for distal tumours when adequate margins can be achieved. Total gastrectomy removes the entire stomach and requires reconstruction with a Roux-en-Y oesophagojejunal anastomosis — connecting the oesophagus directly to the small intestine. Both types are performed with D2 lymphadenectomy — systematic dissection of regional lymph nodes — which is the internationally recommended extent of surgery for curative gastric cancer treatment. Laparoscopic gastrectomy is available for eligible T1/T2 patients.
What is the survival rate for stomach cancer in India?
Survival rates depend heavily on stage at diagnosis. Localised disease (Stage I) has a 5-year survival rate of approximately 60–80% at specialist centres with complete surgical resection and perioperative chemotherapy. Regional disease (Stage II/III, lymph node involvement): approximately 20–40% with modern multimodal treatment. Metastatic disease (Stage IV): 5-year survival of approximately 5–15%; median overall survival has improved to 13–14+ months with combination trastuzumab or nivolumab therapy for appropriate patients. The most important factor is early detection — only 10–20% of Indian stomach cancer cases are diagnosed at an early, curable stage.
What causes stomach cancer?
The single most important and preventable cause of stomach cancer is Helicobacter pylori (H. pylori) infection — responsible for approximately 75–90% of non-cardia gastric cancers. H. pylori infects the stomach lining, causing chronic inflammation that over years progresses to gastric cancer in susceptible individuals. Other important risk factors include: diet high in salted, smoked, and pickled foods; smoking; family history of stomach cancer; chronic atrophic gastritis; previous partial gastrectomy; and hereditary conditions including HDGC syndrome (CDH1 mutations) and Lynch syndrome. H. pylori testing and eradication in high-risk individuals is the most effective preventive strategy currently available.
Can stomach cancer be treated without surgery?
Yes, in specific situations. For Stage 0 and very early Stage IA disease (T1a tumours confined to the mucosa), endoscopic submucosal dissection (ESD) can achieve curative resection without any surgical incision, preserving the entire stomach. For advanced or metastatic disease not amenable to surgery, systemic chemotherapy combined with trastuzumab (HER2+) or nivolumab (PD-L1 CPS ≥5) is the standard treatment and can significantly extend survival. Radiation therapy is used for locally advanced unresectable disease and palliation. For gastric MALT lymphoma, H. pylori eradication alone can cure the cancer without any surgery or chemotherapy. CION's tumour board evaluates every patient for non-surgical options before recommending gastrectomy.
What is the role of H. pylori in stomach cancer?
Helicobacter pylori is a bacterium that infects the stomach lining and is classified as a Class I carcinogen by the WHO. It causes chronic gastritis that progressively damages the stomach lining over years, passing through stages of atrophic gastritis, intestinal metaplasia, and dysplasia before cancer develops. H. pylori is responsible for approximately 75–90% of non-cardia gastric cancers. India has one of the highest H. pylori infection rates globally (50–80% of adults), making it a critical public health concern in Hyderabad and across Telangana. The crucial message: H. pylori can be tested for (urea breath test, stool antigen test, or endoscopic biopsy) and cured with a 10–14 day antibiotic regimen. Treating H. pylori significantly reduces gastric cancer risk and can cure early gastric MALT lymphoma.
What is HER2-positive stomach cancer?
HER2 (Human Epidermal Growth Factor Receptor 2) is a protein that promotes cancer cell growth when overexpressed. Approximately 15–20% of gastric adenocarcinomas are HER2-positive. This is important because HER2-positive gastric cancer responds to trastuzumab (Herceptin) — a monoclonal antibody that binds to the HER2 receptor and blocks tumour growth signals. When trastuzumab is added to platinum-based chemotherapy as first-line treatment, it improves median overall survival compared to chemotherapy alone (ToGA trial data). HER2 testing by IHC and FISH should be performed on all patients with advanced or metastatic gastric cancer before first-line treatment is selected. CION performs HER2 testing as standard workup for all advanced gastric cancer cases.
Can I get a second opinion before stomach cancer surgery?
Absolutely — and for stomach cancer, it is strongly advisable. The decision between perioperative chemotherapy first vs upfront surgery is clinically significant for Stage II/III disease; the choice between subtotal and total gastrectomy has long-term nutritional implications; and many patients are not offered ESD for early-stage disease when they are eligible. CION offers a dedicated Second Opinion service where our multidisciplinary tumour board reviews your endoscopy findings, imaging, pathology, and existing treatment recommendation before advising on the optimal approach. If you have been diagnosed with Stage II or Stage III stomach cancer and surgery has been recommended without pre-operative chemotherapy, a second opinion is strongly advised.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.