Intestinal Cancer Treatment in Hyderabad — Expert Oncology Care Across 7 Locations
When people hear 'intestinal cancer' or 'bowel cancer,' they often picture one disease. In reality, the intestinal tract has two very different sections — the small intestine and the large intestine (colon and rectum) — and cancers in each area are different diseases with different causes, different ways of being found, and different treatments. At CION, our gastrointestinal oncology team treats the full range — from rare small intestine cancers that need specialist diagnostic tools to colon cancer surgery and chemotherapy — across 7 Hyderabad locations, backed by NABH accreditation and NCCN-protocol care.
4 distinct cancer types treated correctly — glandular, neuroendocrine, GIST, lymphoma — each needs a different pathway
Specialist diagnostic pathway — capsule endoscopy + double balloon enteroscopy for small bowel cancers standard cameras can't see
Whipple-capable surgical team — for cancers in the duodenum (first section of small intestine)
Monthly injection therapy for neuroendocrine tumours — octreotide / lanreotide controls symptoms and slows growth
4.8 · 800+ Google reviews · 15,000+ patients treated
17+
Cancer Specialists on Panel
96.9%
Breast Cancer Survival Rate*
15,000+
Patients Treated
4.8★
Google Rating (800+ reviews)
Written by Dr. Sridhar Kamani
Surgical Oncologist · MBBS · MS General Surgery · DrNB Surgical Oncology · CION Cancer Clinics, Hyderabad
Medically reviewed by Dr. Naresh Gundu — Medical Oncologist · MBBS, Guntur Medical College · MD General Medicine, Andhra Medical College. Last reviewed: 20 May 2026.
Understanding Intestinal Cancer
Small Intestine, Large Intestine — Understanding Which Part Is Affected
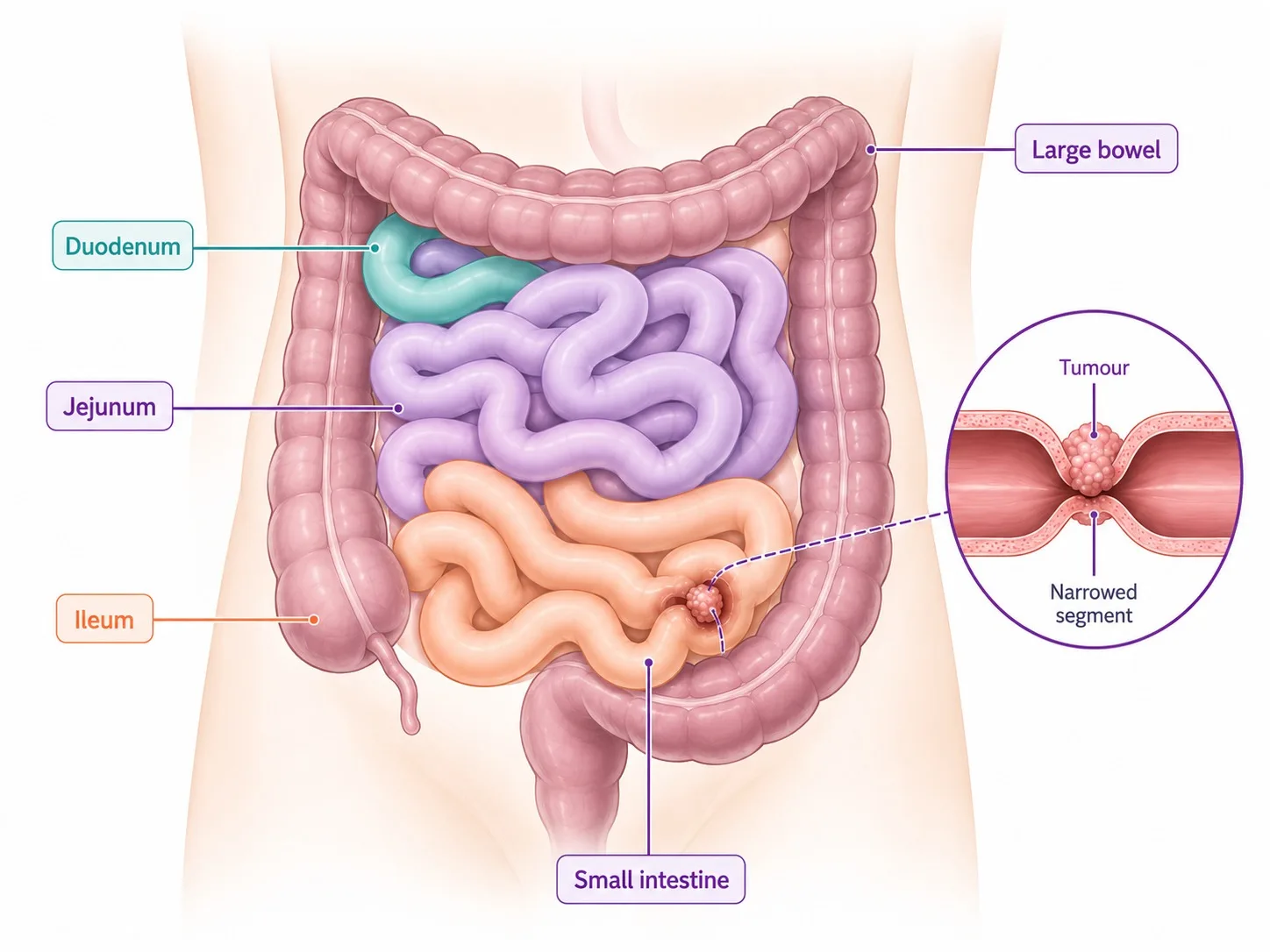
The small intestine is long and coiled — separate from the colon. Tumours here typically cause blockage rather than bleeding.
The intestines are the long tube through which food passes after leaving your stomach. They have two main sections — and cancers in each behave very differently:
The small intestine — about 5 to 6 metres long; divided into three parts (the duodenum just after the stomach, the jejunum in the middle, and the ileum at the end). It absorbs most of the nutrients from digested food. Cancer here is rare — it makes up only about 1 to 3% of all bowel cancers — but it includes several very different types that are often diagnosed late because they are so hard to spot.
The large intestine (colon) — the shorter, wider section that absorbs water before waste passes out of the body. Colon cancer is one of the most common cancers in the world and in India, and is much better understood than small bowel cancer.
The rectum — the last 12 to 15 centimetres before the anus. Rectal cancer shares risk factors with colon cancer but is treated very differently. CION has a dedicated rectal cancer treatment page with full information on that pathway.
Some intestinal cancers are straightforward to diagnose; others can hide undetected for years because the area they grow in cannot be seen by a standard camera examination. The right diagnostic pathway — and the right treatment — depends entirely on which part of the intestine is affected.
Did You Know?
Small intestine cancer is so rare that many people — and even some doctors — never encounter it. One reason it is so uncommon is that food moves quickly through the small intestine, limiting how long any harmful substances stay in contact with the bowel wall. But when it does occur, it can go undetected for a long time because the small intestine cannot be checked with a standard camera test.
Risk Factors
What Increases the Risk of Intestinal Cancer?
Risk Factors for Small Intestine Cancer
Unlike colon cancer, small intestine cancer is not mainly linked to diet. The biggest risk factors are conditions that cause long-term inflammation or irritation of the small bowel lining, and inherited family conditions that affect the whole digestive tract:
Crohn's disease — a long-term inflammatory bowel condition that significantly raises the risk of cancer in the small intestine, particularly in the last section (the ileum).
Celiac disease — an immune reaction to gluten that damages the small intestine; if left untreated for years, it is associated with a rare type of bowel lymphoma (a cancer of the immune cells lining the gut).
Lynch syndrome — an inherited condition caused by a faulty gene that runs in families; it significantly increases the lifetime risk of cancers in both the small bowel and the colon. A simple blood test can check for the faulty gene.
Familial Adenomatous Polyposis (FAP) — an inherited condition causing hundreds of polyps (small growths) to develop throughout the bowel, particularly in the colon but also in the first part of the small intestine (the duodenum). These polyps can turn cancerous if not monitored and removed.
Peutz-Jeghers syndrome — a rare inherited condition causing polyps to grow throughout the small and large intestine; also causes distinctive brown spots on the lips and inside the mouth. People with this condition need regular bowel monitoring from a young age.
Risk Factors for Colon Cancer
Diet high in red and processed meat (beef, lamb, sausages, bacon) and low in fibre — consistently linked to higher colon cancer risk.
Being overweight, inactive, or spending most of the day sitting.
Long-term inflammatory bowel disease — ulcerative colitis or Crohn's disease that affects the large intestine.
Bowel polyps — small benign growths in the colon lining; most colon cancers begin this way over many years; colonoscopy finds and removes them before they turn cancerous.
A close family member (parent, sibling, or child) who has had colon cancer.
Lynch syndrome and FAP — inherited conditions causing a very high lifetime colon cancer risk.
Being over 50 years old — risk increases significantly with age; colonoscopy screening is recommended from this age.
Smoking and drinking alcohol heavily over many years.
If you have a family member diagnosed with colorectal cancer — particularly before age 60 — speak to a CION oncologist about genetic testing for Lynch syndrome. Identifying this hereditary condition can guide screening for you and other family members before cancer develops.
Symptoms
What Are the Warning Signs of Intestinal Cancer?
The symptoms depend on which part of the intestine is affected. Many overlap with far more common and less serious conditions — which is one reason both types of intestinal cancer can be missed early on.
Small Intestine Cancer Warning Signs
Stomach cramping or pain that keeps coming back — often vague, around the middle of the abdomen.
Feeling sick (nausea) and vomiting — particularly if the cancer has grown large enough to partially block the bowel.
Blood in the stool — may appear as dark red blood or as very dark, tarry-looking stools from bleeding higher up in the gut.
Unexplained weight loss — losing weight without trying, often alongside a drop in appetite.
Tiredness and weakness from anaemia — slow bleeding from a tumour can cause a low blood count that leaves patients feeling permanently exhausted even without visible bleeding.
Yellowing of the skin and eyes (jaundice) — specifically for cancers that grow near the opening where the bile duct enters the small intestine, which can block the flow of bile.
Flushing, loose stools, and stomach cramps — sudden redness of the face and neck can be a sign of a type of small intestine cancer called a neuroendocrine tumour, which releases hormones into the bloodstream.
Colon Cancer Warning Signs
A persistent change in your bowel habits — diarrhoea, constipation, or stools that are narrower than usual, lasting more than 2 to 4 weeks.
Blood in or on the stool.
Persistent bloating, gas, or stomach discomfort.
Feeling that your bowel has not emptied completely after a motion.
Unexplained weight loss and tiredness.
Anaemia (a low blood count) without an obvious cause — from slow, hidden bleeding from a tumour.
Don't dismiss blood in the stool or a persistent change in bowel habit. In any adult over 40, blood in the stool, unexplained anaemia, or a lasting change in how the bowel works deserves specialist evaluation. These symptoms are often caused by something other than cancer — but they always deserve investigation.
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the Specialists
Senior GI oncology specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Speak to an Intestinal Cancer Specialist Today
Whether you've been diagnosed with small bowel cancer, colon cancer, a neuroendocrine tumour, or a GIST — same-week appointments across 7 Hyderabad locations.
Why Small Intestine Cancer Is Hard to Find — And How We Find It
The small bowel is hard to reach, so we use specialised tools — capsule endoscopy and CT/MR enterography — to find and map the tumour.
Colon cancer is relatively straightforward to diagnose: a camera examination of the large bowel (colonoscopy) can see the entire colon, and a small tissue sample is taken at the same time. Small intestine cancer is far harder to detect — and this is why it is so often found late.
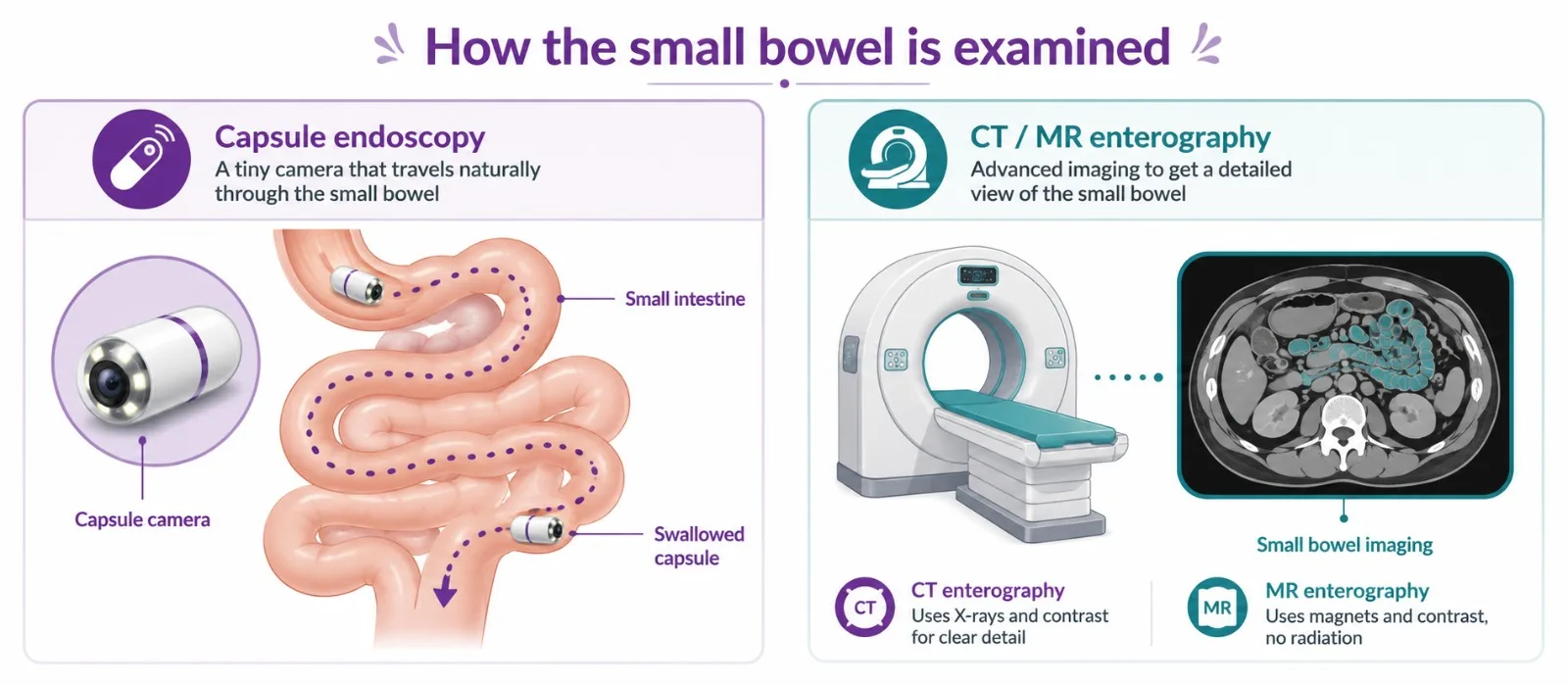
A standard stomach camera reaches only the very first section of the small intestine. A standard colonoscopy reaches the colon and only a very short section of the last part of the small intestine. The 5 to 6 metres in between — where most small bowel cancers grow — cannot be seen by either. Two specialist tools bridge this gap:
Swallowing a Camera Pill (Capsule Endoscopy)
The patient swallows a small capsule — about the size of a large vitamin tablet — that contains a tiny camera and a transmitter. As the capsule travels naturally through the small intestine over the course of the day, it takes thousands of photographs of the bowel lining, which are transmitted wirelessly to a recording device worn on the patient's belt. The images are reviewed by a specialist who looks for any suspicious lesion, area of bleeding, or abnormal growth. The process is painless, does not require sedation, and the capsule passes naturally.
Getting a Sample from the Small Bowel (Double Balloon Enteroscopy)
When the camera pill identifies a suspicious area, a second specialist procedure is used to actually reach that part of the small intestine, look at it directly, and take a tissue sample for testing. This uses a specially designed flexible tube with two small balloons that grip the bowel wall and allow the scope to be pushed progressively deeper — from either the mouth or the rectum — until the target area is reached. It is done under sedation and allows the doctor to take a biopsy from any location in the small bowel. It is currently the best available tool for confirming small intestine cancer.
A Specialised CT Scan
A specially designed CT scan, taken after the patient drinks a large amount of liquid that fills and expands the small bowel, gives doctors a detailed image of the small intestinal wall. This helps identify tumour masses, check nearby lymph nodes, and assess whether the cancer has spread.
Diagnosing Colon Cancer
Colon cancer diagnosis is more straightforward: a colonoscopy camera examines the entire colon and takes a tissue sample from any suspicious area (watch a Mayo Clinic overview of colorectal cancer). A CT scan of the chest and abdomen checks whether cancer has spread. A blood test called CEA — which measures a substance that colon cancer cells release into the bloodstream — helps monitor how well treatment is working and checks for recurrence after surgery.
Subtypes Matter
The Four Main Types of Small Intestine Cancer
Small intestine cancer is not one disease — it is four distinct conditions that happen to grow in the same part of the body. Getting the right treatment depends on correctly identifying which type is present from the pathology report.
Most common type
Type 1 — Glandular Cell Cancer
Grows from the cells that line the inner wall of the bowel. It behaves similarly to colon cancer and is treated the same way — surgery to remove the affected section of bowel, followed by chemotherapy to reduce the risk of the cancer coming back. Cancers in the very first part of the small intestine (the duodenum), near where the bile duct opens in, may require a more complex operation called a Whipple procedure — the same operation used for pancreatic cancer of the head of the pancreas.
Slow-growing · hormone-producing
Type 2 — Neuroendocrine Tumours (Carcinoids)
Grow from hormone-producing cells scattered throughout the small bowel. Typically slow-growing — sometimes present for years before causing symptoms. They become noticeable when they spread to the liver and release hormones, causing carcinoid syndrome: sudden flushing of the face and neck, repeated watery diarrhoea, stomach cramping, and sometimes wheezing. For tumours that cannot be fully removed, monthly octreotide or lanreotide injections control symptoms dramatically and slow tumour growth. Many patients live 10 years or more with the right management.
Bowel wall tumour
Type 3 — Stromal Tumours (GISTs)
Grow from the muscle layer of the small intestine wall rather than the inner lining — fundamentally different from the other types. Standard chemotherapy does not work against them. Instead, they are treated with a daily tablet called imatinib, which targets the specific gene abnormality driving the tumour's growth. If you have been diagnosed with a GIST and are being offered conventional bowel cancer chemotherapy, this needs to be reviewed — the treatment pathway is different.
Immune-cell cancer
Type 4 — Lymphoma of the Small Intestine
A cancer of the immune cells within the bowel lining. The most common subtype is B-cell lymphoma (treated with chemotherapy combinations similar to those used for lymphoma elsewhere in the body). Less commonly, a type linked to untreated celiac disease. Lymphoma of the small bowel is treated primarily with chemotherapy rather than surgery. Surgery is reserved for complications such as a blocked or perforated bowel.
Staging & Outlook
How Advanced Is the Cancer? — Staging and Survival
Small intestine cancer is described in four stages based on how deeply it has grown and whether it has spread beyond the bowel. Stage at diagnosis is the most important factor in determining what treatment is possible and what the outlook is.
Stage
What it means
Typical plan
5-yr outlook (NCCN-grade care)
Stage I
In the bowel wall only · No nodes, no distant spread
Surgery to remove the affected section + nearby lymph nodes
60–80%
Stage II
Through the full bowel wall · No nodes, no distant spread
Surgery + chemotherapy after the operation
40–60%
Stage III
Reached nearby lymph nodes · No distant spread
Surgery + chemotherapy after the operation
25–45%
Stage IV
Spread to distant organs (liver, lungs, or other organs)
Chemotherapy + targeted medicines; surgery for bowel blockage if needed
5–15%
*5-year survival figures are for the glandular cell type of small intestine cancer at specialist centres. The slow-growing neuroendocrine type has significantly better outcomes at the same stages. Individual results depend on how well the cancer responds to treatment and the overall health of the patient.
Treatment — Small Intestine
Treatment for Small Intestine Cancer at CION
Surgery
Surgery is the only way to cure small intestine cancer that has not spread beyond the bowel. CION's surgical oncology team performs the right operation based on where the cancer is located:
For cancers in the middle or lower small intestine — the affected section of bowel is removed along with a clear margin of healthy bowel on each side and the nearby lymph nodes. The two remaining ends of the intestine are then joined back together. Depending on the patient, this can be done through a large incision or through smaller keyhole cuts (laparoscopically).
For cancers in the first section of the small intestine (the duodenum) — this area is very close to the head of the pancreas and the bile duct opening, so a more complex operation called a Whipple procedure is usually required. This is the same operation performed for pancreatic cancer in that area, and it involves removing the duodenum, the head of the pancreas, part of the bile duct, and the gallbladder, before reconnecting the digestive system. It is one of the most complex abdominal operations performed in oncology and requires an experienced surgical oncology team.
Chemotherapy After Surgery
After surgery, chemotherapy is recommended for patients with higher-risk tumours — where the cancer had grown through the full thickness of the bowel wall, or where nearby lymph nodes were involved. A combination of chemotherapy medicines is given as a drip every two weeks (FOLFOX), or as a similar combination where one of the medicines is an oral tablet taken at home (CAPOX). The aim is to destroy any microscopic cancer cells that may have been left behind and reduce the chance of the cancer coming back. CION's medical oncology team delivers this in a comfortable day-care setting, with regular monitoring throughout.
Treatment for Slow-Growing Neuroendocrine Tumours (NETs)
Surgery — the first treatment for tumours that can be removed; even when the cancer has spread to the liver, removing as much of it as possible helps control hormone symptoms and improves survival.
Monthly injections (octreotide or lanreotide) — for tumours that cannot be fully removed or that have spread; these once-monthly injections keep hormone symptoms under control (stopping or dramatically reducing flushing and diarrhoea) and slow the tumour's growth. Many patients remain on them for years with a good quality of life.
Everolimus — a daily tablet that slows tumour growth further; used when the monthly injections alone are no longer sufficient.
Targeted radiation treatment — for patients whose tumour cells have specific receptors on their surface, a specialist treatment can deliver radioactivity directly to tumour cells wherever they are in the body; arranged through CION's specialist referral network.
Treatment — Colon Cancer
Colon Cancer Treatment at CION
Colon cancer — cancer of the large intestine — is one of the most treatable gastrointestinal cancers when found early. CION's colorectal oncology team manages all stages of colon cancer.
Surgery to Remove Colon Cancer
Surgery is the main treatment for colon cancer that has not spread to distant organs. The operation involves removing the section of colon containing the tumour along with a healthy margin on each side and the nearby lymph nodes, then reconnecting the remaining colon. The type of operation depends on which part of the colon is affected.
Keyhole (laparoscopic) surgery — the preferred approach for eligible patients; smaller cuts, less pain, faster recovery, and equivalent cancer outcomes to open surgery.
Open surgery — used when the cancer is large, in a difficult location, or when a previous abdominal surgery makes keyhole access more complex.
Emergency stenting — for patients with a blocked colon caused by cancer; a small metal tube is placed inside the bowel to open the blockage, avoiding emergency surgery and allowing the patient to be stabilised before a planned operation.
Removal of the entire large bowel — occasionally needed for patients with an inherited condition causing cancer throughout the colon (such as FAP or Lynch syndrome) or for cancers in multiple sites.
Chemotherapy and Targeted Treatment for Colon Cancer
After surgery for more advanced colon cancer, a 6-month course of chemotherapy (given as a drip every 2 weeks or as tablets combined with a shorter drip) significantly reduces the chance of the cancer coming back. For colon cancer that has spread to other organs — most commonly the liver or lungs — chemotherapy is the main ongoing treatment, often combined with a targeted medicine chosen based on a molecular test done on the tumour tissue.
Molecular testing of the tumour — a test done on the tissue removed by surgery or biopsy; it checks for specific gene changes that determine which additional medicines are likely to work. Patients whose tumour does not carry a certain gene change can benefit from a targeted medicine that blocks cancer cell growth signals. Patients whose tumour shows a defect in how its DNA repairs itself (MSI-H/dMMR) may respond very well to immunotherapy rather than standard chemotherapy.
Anti-blood vessel medicines — added to chemotherapy to cut off the blood supply the tumour needs to grow.
Immunotherapy — for the specific group of patients whose tumour carries a DNA repair defect; this has been shown to work better than standard chemotherapy as a first treatment in this group.
For rectal cancer specifically — including the decision about whether chemotherapy and radiation are given before surgery, and whether surgery can be avoided entirely in some patients — see CION's dedicated Rectal Cancer Treatment page.
Hereditary Conditions
Is Your Bowel Cancer Hereditary? — Protecting Your Family
A meaningful proportion of intestinal cancers — both small bowel and colon — run in families because of inherited gene changes. At CION, we offer genetic testing to patients who are diagnosed with bowel cancer at a young age, have had multiple bowel cancers, or have several family members affected. If a hereditary condition is confirmed, close family members can be tested and monitored — sometimes catching cancer early enough to prevent it altogether.
Lynch syndrome — the most common hereditary bowel cancer condition; caused by a faulty gene inherited from a parent; significantly raises lifetime risk of colon cancer, small bowel cancer, and several other cancers. A simple test of the tumour tissue can flag this at the time of diagnosis, after which a blood test confirms whether the gene fault is inherited. Family members who carry the gene can start regular bowel camera monitoring years earlier than the general population.
Familial Adenomatous Polyposis (FAP) — causes hundreds of small polyp growths in the colon from early adulthood; without management, these almost always become cancerous. Also causes polyps in the first part of the small intestine that need monitoring. People with FAP are usually identified in childhood or early adulthood through family testing.
Peutz-Jeghers syndrome — causes multiple polyps throughout the intestinal tract, together with distinctive dark spots on the lips and inside the mouth; requires lifelong monitoring of the bowel at specialist centres.
Celiac disease — not a genetic cancer syndrome in itself, but long-standing untreated celiac disease is associated with a small increased risk of a rare type of intestinal lymphoma; the risk largely disappears with strict adherence to a gluten-free diet.
If you have been diagnosed with bowel cancer before the age of 50, if multiple family members have had bowel or related cancers, or if you have one of the conditions above, speak to a CION oncologist about genetic counselling and testing for yourself and your family.
How Decisions Are Made
Every Case Reviewed by a Team Before Treatment Begins
Intestinal cancer covers a wide range of very different diseases. The treatment decisions — particularly for small intestine cancer, where the type of cancer fundamentally changes the treatment — require specialist input from surgeons, medical oncologists, and gastroenterologists together. At CION, every case is reviewed by our multidisciplinary team before any recommendation is made:
Identifying the exact type of small intestine cancer from the pathology report — each type has a completely different treatment plan.
Arranging a camera pill examination and specialist bowel scope for lesions that cannot be reached by standard endoscopy.
Choosing the right surgical approach — standard bowel resection or the more complex Whipple procedure for cancers in the first part of the small intestine.
Molecular testing of the tumour to identify which chemotherapy and targeted medicines will work best.
Monthly injection therapy for slow-growing neuroendocrine tumours — managing symptoms and slowing tumour growth.
Genetic testing offered to appropriate patients and discussion of family screening implications.
Colon cancer staging and chemotherapy sequencing across the multidisciplinary team.
Link to CION's Rectal Cancer Treatment pathway for rectal-specific cases.
NCCN and ESMO evidence-based protocol alignment across all subtypes.
Digital coordination across all 7 Hyderabad locations.
Why Patients Choose CION for Intestinal Cancer Treatment in Hyderabad
Sixteen reasons our patients pick CION — each subtype treated with the right pathway, specialist diagnostic tools, and a multidisciplinary tumour board reviewing every case before treatment.
1,000+ Cancer Cases Treated Every Year
Across the CION network
7 locations across Hyderabad
Kukatpally, Kompally, Ameerpet, Tolichowki, MasabTank, L.B. Nagar, Banjara Hills — 70% less travel than single-centre hospitals
5-Star NABH Accredited
Cancer Care Institutes
NCCN & ESMO Protocol Adherence
Across all intestinal cancer types
Each subtype treated correctly
NETs, GISTs, lymphoma, and glandular cancer — each follows a completely different pathway
Specialist diagnostic pathway
Capsule endoscopy & double balloon enteroscopy for small bowel cancers standard cameras miss
Whipple-capable surgical team
For cancers in the first part of the small intestine (duodenum)
Not conventional chemotherapy — the wrong pathway is common elsewhere
Molecular testing as standard
For all advanced tumours — RAS, BRAF, MSI-H/dMMR — to choose the most effective combination
Genetic counselling
For Lynch syndrome, FAP, Peutz-Jeghers & other hereditary conditions — with family testing guidance
Dedicated Second Opinion service
Free written review of your endoscopy, imaging, and pathology
EMI facility
Flexible payment options for all patients
4.8 / 5 Google rating
Across 1,000+ patient reviews
India's fastest-growing cancer network
35+ centres across Telangana and Andhra Pradesh
Digital coordination across centres
Reports and tumour-board decisions follow you across all 7 Hyderabad locations
Transparent Costs
Intestinal Cancer Treatment Cost in Hyderabad
Costs vary depending on which part of the intestine is affected, the extent of surgery required, and whether ongoing chemotherapy or other medicines are needed:
Treatment
Approx. Cost (INR)
Notes
Small Intestine Surgery (standard section removal)
₹2,00,000 – ₹5,00,000
Varies by extent of surgery and recovery
Whipple Procedure (for first section of small intestine)
₹4,00,000 – ₹12,00,000
Complex surgery; ICU stay included
Colon Cancer Surgery (keyhole)
₹2,50,000 – ₹6,00,000
Varies by how much of the colon is removed
Chemotherapy Drip (per course)
₹25,000 – ₹80,000
Given every 2 weeks; 12 courses standard for after-surgery treatment
Targeted Medicine (per course)
₹60,000 – ₹1,80,000
Added to chemotherapy based on tumour testing
Monthly Injection for Neuroendocrine Tumours
₹25,000 – ₹70,000
Ongoing monthly injection; manages symptoms and slows growth
Immunotherapy (per course)
₹1,00,000 – ₹2,50,000
For specific tumour type with DNA repair defect (MSI-H/dMMR)
Full Treatment Pathway
₹2,00,000 – ₹15,00,000+
Depending on type, stage, and duration of treatment
Costs are indicative. A personalised cost estimate is provided following your initial oncology consultation at CION.
Financial Support Options
EMI Facility — flexible instalment-based payment options available for all patients.
Private Health Insurance — CION works with all major TPAs for cashless hospitalisation; targeted therapy and immunotherapy coverage varies by insurer.
Did You Know?
Not all bowel cancers are the same — and the treatment depends entirely on the type. A slow-growing neuroendocrine tumour of the small bowel is managed with monthly injections, not standard chemotherapy. A stromal tumour of the bowel wall (GIST) is treated with a daily tablet called imatinib, not surgery alone. A bowel lymphoma is treated with a chemotherapy combination, not bowel removal. Getting the correct diagnosis from a pathologist experienced in bowel cancers is the single most important first step in the right treatment journey.
Next Step
Book a 45-Minute Consultation — No Rushed Decisions
Bring your reports. Our oncologists will walk you through the diagnosis type, staging, treatment options, expected costs, and quality-of-life impact — clearly and honestly.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
Successful Chemotherapy & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan
Watch video →
Successful Chemotherapy Done by Dr. C Raghavendra Reddy
Watch video →
Surgery, Chemo & Radiation Done by Dr. Imaduddin, Dr. Vinay, Dr. Owais, Dr. Kirti
Watch video →
Successful Radical Thymectomy Done by Dr. Mohammed Imaduddin & Dr. Vinay Mamidala
Watch video →
Successful Surgery Done by Dr. Rajender Byshetty
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Surgery Done by Dr. Imad, Dr. Vinay, Dr. Owais & Dr. Raghavendra
Watch video →
Successful Chemo & Radiation Done by Dr. Owais Mohammed & Dr. Kirti Ranjan Mohanty
Watch video →
Successful Breast Cancer Surgery Done by Dr. Imaduddin Mohammed & Dr. Vinay Mamidala
Watch video →
Successful Chemotherapy Done by Dr. Bharati Devi Gorantla
Watch video →
Successful Chemo & Surgery Done by Dr. Owais Mohammed & Dr. Imaduddin Mohammed
Watch video →
Successful Chemotherapy Done by Dr. Gundu Naresh
Watch video →
Successful Bone Marrow Transplantation - Neuroblastoma
Watch video →
Successful Surgery & Chemo - Carcinoma of Caecum
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Surgery by Dr. Mohammed Imaduddin
Watch video →
Successful Bone Marrow Transplantation
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Oral chemotherapy & mastectomy surgery
Watch video →
Successful Chemotherapy
Watch video →
Successful Buccal Mucosa Surgery
Watch video →
Successful Complex Surgery Mandibulectomy Reconstruction
Intestinal Cancer Treatment — Frequently Asked Questions
What are the symptoms of intestinal cancer?
Small intestine cancer often causes recurring stomach cramps, nausea, dark or tarry stools from internal bleeding, unexplained weight loss, and persistent tiredness from anaemia. Cancers near the bile duct opening may cause yellowing of the skin. Slow-growing neuroendocrine tumours can cause sudden flushing and loose stools. Colon cancer typically presents with a change in bowel habits, blood in the stool, bloating, or weight loss. Any blood in the stool or lasting change in bowel habit in an adult over 40 should be investigated.
Is intestinal cancer curable?
Yes — particularly when found early. Small intestine glandular cancer caught before it spreads has 5-year survival rates of 60–80% with surgery and chemotherapy. Colon cancer at Stage I is curable in over 90% of patients. Slow-growing neuroendocrine tumours of the small bowel often allow patients to live 10 or more years even after spread, with monthly injection treatment keeping the disease controlled. Early detection through bowel screening is the single most important factor.
What is small intestine cancer?
Small intestine cancer grows in the 5 to 6 metre section of gut between the stomach and the large intestine. It is rare — only 1 to 3% of all bowel cancers. There are four main types: glandular cancer (most common, treated like colon cancer); slow-growing hormone-producing tumours called neuroendocrine tumours (managed with monthly injections); stromal tumours of the bowel wall called GISTs (treated with a specific daily tablet, not standard chemotherapy); and lymphoma of the bowel lining (treated with chemotherapy). Each requires a completely different approach.
What causes intestinal cancer?
Small intestine cancer is mainly linked to long-term bowel inflammation (Crohn's disease) or inherited family conditions — Lynch syndrome, Familial Adenomatous Polyposis, and Peutz-Jeghers syndrome. Untreated celiac disease is also associated with a rare type of bowel lymphoma. Colon cancer is primarily caused by diet (high red and processed meat, low fibre), obesity, inactivity, inflammatory bowel disease, and family history. Age matters significantly for both — risk rises sharply after 50.
How is intestinal cancer diagnosed?
Colon cancer is diagnosed by colonoscopy — a camera passed through the bowel — with a tissue sample taken at the same time. The small intestine cannot be seen by standard cameras, so two specialist tools are used: a camera pill the patient swallows, which photographs the entire small bowel as it travels through; and a specialist scope that reaches the small bowel directly for a biopsy. A specialist CT scan with the bowel filled with liquid gives detailed images. For neuroendocrine tumours, a nuclear medicine scan locates where the cancer has spread.
What is the difference between small intestine and colon cancer?
Small intestine cancer is rare, hard to detect without specialist tools, and includes subtypes — neuroendocrine tumours and stromal tumours — that do not occur in the colon. Colon cancer is common, detected easily by colonoscopy, and is primarily one type (glandular). Surgery for small bowel cancer can range from a section removal to a complex Whipple procedure near the bile duct. Both use chemotherapy, but which additional medicines are appropriate depends on a test done on the tumour tissue.
What is the survival rate for intestinal cancer?
Small intestine glandular cancer: Stage I 60–80%; Stage II 40–60%; Stage III 25–45%; Stage IV 5–15%. Slow-growing neuroendocrine tumours have a much more favourable outlook — many patients live 10 or more years on monthly injections. Colon cancer: Stage I over 90%; Stage II 75–85%; Stage III 50–70%; Stage IV 15–30% overall, though patients with spread limited to the liver that can be surgically removed do considerably better.
Can intestinal cancer be treated without surgery?
Yes, for some types. Slow-growing neuroendocrine tumours that have spread are often managed for years with monthly injections, controlling symptoms and slowing growth without any operation. Stromal tumours of the bowel wall (GISTs) that cannot be removed are treated with a daily targeted tablet. Bowel lymphoma is treated with chemotherapy, not surgery. Advanced colon cancer is managed with chemotherapy and targeted medicines; surgery on the liver is added for selected patients. CION's team always evaluates non-surgical options before recommending an operation.
What is the cost of intestinal cancer treatment in Hyderabad?
Standard small intestine surgery: ₹2,00,000–₹5,00,000. Whipple procedure (first section of small intestine): ₹4,00,000–₹12,00,000. Keyhole colon surgery: ₹2,50,000–₹6,00,000. Chemotherapy: ₹25,000–₹80,000 per cycle. Monthly injections for neuroendocrine tumours: ₹25,000–₹70,000 per month. Targeted medicines: ₹60,000–₹1,80,000 per course. A personalised cost estimate is provided after your initial consultation at CION. EMI options are available.
Can I get a second opinion for intestinal cancer?
Absolutely. A second opinion is especially valuable if: the type of small intestine cancer has not been clearly confirmed — each type needs a completely different treatment; colon surgery has been recommended and you want to understand whether a keyhole approach is suitable; or advanced intestinal cancer has been declared untreatable without a tumour tissue test, because certain genetic changes in the cancer can open treatment options that standard chemotherapy cannot. CION offers a dedicated Second Opinion service.
Need a Second Opinion?
Free consultation with a specialist. No commitment.