
CION 1-year survival*
80.0%
India accounts for approximately one-third of the world's oral cancer cases — a burden driven overwhelmingly by tobacco use in its many forms: cigarettes, bidis, gutka, pan masala, khaini, and areca nut. In Telangana and Andhra Pradesh, where smokeless tobacco use is particularly prevalent, oral cancer is one of the most commonly diagnosed malignancies. Yet it is also one of the most preventable and, when detected early, one of the most curable cancers in oncology.
India accounts for approximately 30% of all oral cancer cases globally — more than any other country. According to ICMR data, oral cancer is the most common cancer in Indian men and the third most common in Indian women. This disproportionate burden is directly attributable to India's exceptionally high rates of tobacco use — and Telangana sits among the states with the highest smokeless tobacco consumption in the country.
Unlike oral cancers in Western populations — where alcohol and HPV infection are the dominant risk factors — the vast majority of oral cancers in Hyderabad and across Telangana / AP are caused by:
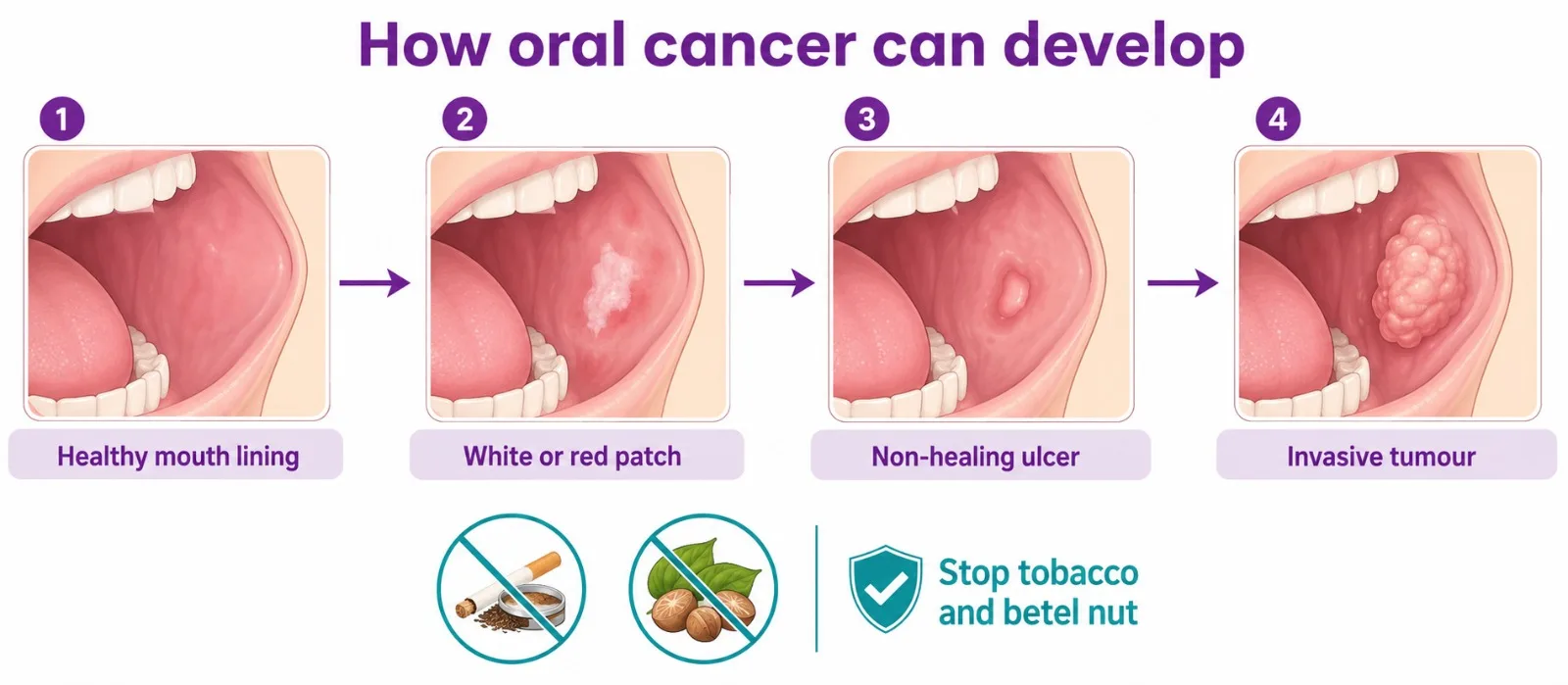
If you use any form of tobacco or areca nut and have any unusual change in your mouth — including a sore that will not heal, a white or red patch, or a lump in the mouth or neck — do not wait. Oral cancers detected at Stage I or Stage II have 5-year survival rates exceeding 80%.
India accounts for approximately one-third of the world's oral cancer cases. The majority are directly caused by tobacco — particularly smokeless tobacco forms like gutka, khaini, and pan masala, which are widely used across Telangana and Andhra Pradesh. Oral cancer is almost entirely preventable — cessation of tobacco and areca nut use eliminates the leading risk.
Oral squamous cell carcinoma (OSCC) accounts for over 90% of all oral cancers. However, the site within the oral cavity significantly affects treatment approach, surgical planning, and functional outcomes. In India, the subsite pattern differs markedly from Western countries due to the dominant role of smokeless tobacco. Tap any subtype to expand.
The buccal mucosa — the inner lining of the cheeks — is the most common oral cancer site in India, directly caused by gutka and khaini placed in the cheek. In Western populations, tongue cancer dominates; in India, buccal mucosa cancer accounts for the plurality of oral cavity cases. It typically presents as an ulcerated lesion, white patch (leukoplakia), or exophytic mass on the inner cheek. Surgical resection with adequate margins and neck dissection is the primary treatment. Reconstruction of large buccal defects requires careful planning to restore chewing and speech function.
The most commonly diagnosed oral cancer globally, and the second most common in India. Arises predominantly on the lateral border and undersurface of the tongue — areas in contact with tobacco and teeth irritation. Tongue cancer has a higher propensity for early cervical lymph node metastasis than most other oral sites, making neck dissection almost always necessary. Reconstruction after partial glossectomy is critical for preserving speech and swallowing. CION's surgical oncology team coordinates tongue cancer treatment in Hyderabad across all 8 locations.
Develops in the soft tissue below the tongue, often associated with tobacco and alcohol. Frequently involves the tongue, lower jaw (mandible), and salivary gland ducts, making complete resection complex. Free-flap reconstruction is commonly required to restore swallowing and speech function after wide resection.
Predominantly squamous cell carcinoma of the lower lip; associated with sun exposure (fair-skinned individuals) and smoking. Excellent prognosis when detected early. Surgical resection with careful reconstruction to preserve lip competence and cosmesis — particularly important for speech, eating, and facial appearance.
Gingival cancers often invade the underlying jawbone (mandible or maxilla) requiring bone resection and titanium plate reconstruction. Hard palate cancers may extend to involve the nasal cavity. Both require careful preoperative imaging and surgical planning to achieve clear margins while preserving function.
Cancers of the oropharynx — base of tongue, tonsils, soft palate, and posterior pharyngeal wall — are anatomically distinct from oral cavity cancers. In India, HPV-16 infection is an increasingly recognised cause of oropharyngeal cancer, particularly in younger, non-tobacco-using patients. HPV-positive oropharyngeal cancer has a significantly better prognosis than tobacco-related disease and may respond differently to treatment — making HPV testing important for all oropharyngeal cancer diagnoses.
Oral cancer is one of the few cancers where self-examination can genuinely save lives — you can watch a Mayo Clinic specialist explain the signs and risk factors of oral cancer. The following warning signs require urgent specialist evaluation — ideally within 2 weeks:
Oral submucous fibrosis (OSMF) — a precancerous condition from areca nut and gutka use causing progressive mouth stiffening and restricted opening — carries a 7–13% lifetime risk of malignant transformation and must be managed by an oncologist, not just a dentist.
The KEYNOTE-048 trial established pembrolizumab as the new first-line standard of care for recurrent or metastatic head and neck squamous cell carcinoma, replacing the previous EXTREME regimen. Patients with PD-L1 CPS ≥20 treated with pembrolizumab monotherapy had a median overall survival of 23.4 months — more than double the 10.7 months achieved with the previous standard. PD-L1 CPS testing at diagnosis is now essential for all recurrent oral cancer patients.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.






Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centreTravelling for treatment? We may have a centre right where you are.
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.


MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)



MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)



MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)







MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationShare your name and number — we'll call you back within 30 minutes to schedule your consultation.
Same-week appointments and a dedicated second-opinion pathway across 8 Hyderabad locations.
An accurate, biopsy-confirmed diagnosis is essential before any treatment begins. CION's diagnostic pathway is thorough, efficient, and aligned with NCCN and ESMO standards.
All suspicious oral lesions require tissue biopsy for histological diagnosis. CION's diagnostic pathway:
Oral cancer is staged using the TNM (AJCC 8th edition) system. Stage at diagnosis is the strongest predictor of outcome and determines the treatment approach.
| Stage | TNM Status | Extent of Disease | 5-Year Survival | Primary Treatment |
|---|---|---|---|---|
| Stage I | T1, N0, M0 | Tumour ≤2cm, no nodes, no spread | 80–90% | Wide local excision; elective neck dissection |
| Stage II | T2, N0, M0 | Tumour 2–4cm, no nodes, no spread | 65–80% | Wide local excision + neck dissection ± adjuvant radiation |
| Stage III | T3 or N1, M0 | Tumour >4cm or single ipsilateral node ≤3cm | 40–60% | Surgery + adjuvant chemoradiation for high-risk features |
| Stage IVA | T4a or N2, M0 | Moderately advanced local / regional disease | 25–40% | Surgery + adjuvant CCRT; or definitive CCRT if unresectable |
| Stage IVB–C | T4b or N3 or M1 | Very advanced local disease or distant spread | 10–20% | Systemic therapy (pembrolizumab ± chemo); palliative CCRT |
5-year survival estimates are for oral squamous cell carcinoma at specialist oncology centres. HPV-positive oropharyngeal cancer carries significantly better prognosis at equivalent stages.
*1-year survival rates for oral cancer patients at CION Cancer Clinics vs the national average reported by ICMR / National Cancer Registry Programme (NCRP). Higher CION outcomes reflect specialist tumour-board care, NCCN-aligned protocols, and integrated reconstructive and rehabilitation pathways.
CION follows NCCN protocol-driven treatment planning for all oral cancer sites and stages. Every case is reviewed by our multidisciplinary tumour board before treatment begins.
Surgery is the primary treatment for most oral cavity cancers. CION's surgical oncology team, led by Dr. Vinay Mamidala, performs the full range of oral cancer surgical procedures.
Removal of the primary tumour with a clear surgical margin of at least 1cm of normal tissue around it. The adequacy of surgical margins is the single most important determinant of local recurrence risk.
Removal of part of the tongue for tongue cancer; the extent depends on tumour size and location. Reconstruction is essential for speech and swallowing preservation — often using a radial forearm free flap.
Removal of part of the lower jaw when bone invasion is confirmed on imaging. Followed by reconstruction with a fibula free flap — the gold standard for restoring mandibular continuity and enabling dental implant placement.
For hard palate or upper gum cancers involving the upper jaw. Preoperative imaging guides the extent of bone resection; reconstruction may involve obturators or composite flaps to restore oral-nasal separation.
Systematic removal of cervical lymph nodes to treat or prevent lymph node spread. Recommended for all T2 and above oral cancers and most T1 tumours with depth of invasion >4mm. Types include selective, modified radical, and radical neck dissection based on clinical nodal status.
Surgical removal of large oral cancers — particularly those involving the tongue, floor of mouth, cheek, or jawbone — leaves significant defects that affect speaking, swallowing, appearance, and quality of life. Microvascular free-flap reconstruction is the gold standard technique for restoring these defects. CION coordinates microvascular free-flap reconstruction for eligible patients through its surgical oncology network.
A free flap involves transferring tissue from a distant donor site on the patient's body to the oral defect. The tissue's artery and vein are reconnected under a microscope (microsurgery) to establish a new blood supply.
Thin, pliable skin and soft tissue from the inner forearm; ideal for tongue, buccal mucosa, and floor-of-mouth reconstruction. Preserves oral mobility and speech function after wide resection.
Bone and overlying skin from the lower leg; the gold standard for mandibular (jaw) reconstruction after segmental mandibulectomy. Allows dental implant placement post-reconstruction.
Versatile large-volume flap from the thigh; used for extensive cheek, floor-of-mouth, or composite defects where a high tissue volume is needed.
Regional pedicled flap for patients not suitable for microvascular reconstruction. Simpler and faster but with less optimal functional outcomes compared to free flaps.
The goal of reconstruction is not just to close the wound — it is to restore the patient's ability to eat, speak, and maintain social interaction. CION's reconstruction planning begins before surgery, in coordination with the surgical and speech rehabilitation teams.
CION's radiation oncology team uses advanced techniques to deliver precise, high-dose radiation to oral cancers while protecting surrounding structures — teeth, salivary glands, jaw, and spinal cord.
For patients after surgery with high-risk pathological features: positive or close surgical margins, lymph node involvement, extranodal extension, perineural invasion, or lymphovascular invasion. Typically 60–66 Gy over 6 weeks.
For locally advanced, unresectable oral and oropharyngeal cancers. Cisplatin-based chemotherapy sensitises cancer cells to radiation. Delivers 70 Gy over 7 weeks; preferred primary treatment for unresectable Stage III/IVA disease.
Shapes the radiation beam to conform precisely to the tumour volume, significantly reducing dose to the parotid glands (reducing xerostomia / dry mouth), spinal cord, and mandible.
Real-time imaging during treatment for daily position verification. Critical for oral and oropharyngeal targets where small movements significantly affect dose accuracy.
For pain control, bleeding, or airway obstruction in advanced disease. Delivered as shorter courses to improve quality of life when curative treatment is not feasible.
For patients with recurrent, locally advanced unresectable, or metastatic oral squamous cell carcinoma, the systemic treatment landscape has been transformed by immunotherapy. CION's medical oncology team delivers these protocols in alignment with current NCCN and ESMO guidelines. Tap any option to expand.
The KEYNOTE-048 trial established pembrolizumab as the new first-line standard of care for recurrent or metastatic head and neck squamous cell carcinoma (including oral cavity), replacing the previous EXTREME regimen (cetuximab + chemotherapy). NCCN Category 1 recommendations:
PD-L1 CPS testing is performed at CION on all biopsy tissue from recurrent or metastatic oral cancer to determine pembrolizumab eligibility and the optimal first-line regimen.
Cetuximab — a monoclonal antibody targeting the epidermal growth factor receptor (EGFR) — is used in two clinical settings for oral and oropharyngeal cancers:
The chemotherapy backbone for oral cancer at CION:
Surgery to the tongue, floor of mouth, soft palate, or oropharynx — and radiation therapy to the same areas — can significantly affect the ability to speak clearly and swallow safely. These functional changes are the most important quality-of-life concerns for most oral cancer patients. At CION, speech and swallowing rehabilitation is a structured component of every oral cancer treatment plan:
Oral cancer management requires the tightest multidisciplinary coordination in oncology — surgical oncology, radiation oncology, medical oncology, reconstructive surgery, speech therapy, dental rehabilitation, and nutrition must all contribute. At CION, every oral cancer case is reviewed by our tumour board:
Thirteen reasons our patients pick CION — full surgical spectrum, KEYNOTE-048 immunotherapy, free-flap reconstruction, and NCCN protocols across 8 Hyderabad locations.
1,000+ Oral Cancer Cases / Year
8 locations across Hyderabad
5-Star NABH Accredited
NCCN & ESMO Protocol Adherence
Experienced surgical oncology team
IMRT & IGRT radiation
Dedicated speech & swallowing rehabilitation
Multidisciplinary tumour board
Full integrative support
Dedicated Second Opinion service
EMI Facility
4.8 / 5 across 1,000+ patient reviews
15,000+ patients treated
The cost of oral cancer treatment in Hyderabad varies by stage, site, surgical extent, and whether reconstruction is required. The reference ranges below are based on current Hyderabad market data. A personalised estimate is provided after your initial oncology consultation at CION.
| Treatment | Approx. Cost (INR) | Notes |
|---|---|---|
| Wide Local Excision + Neck Dissection | ₹1,50,000 – ₹4,00,000 | Varies by tumour size and neck dissection extent |
| Wide Excision + Reconstruction (pedicled flap) | ₹2,50,000 – ₹5,00,000 | Pectoralis major myocutaneous flap |
| Resection + Free-Flap Reconstruction | ₹4,00,000 – ₹8,00,000 | Radial forearm, ALT, or fibula flap; microsurgery premium |
| Mandibulectomy + Fibula Free Flap | ₹6,00,000 – ₹12,00,000 | Jaw resection + bone reconstruction; highest complexity |
| Radiation Therapy — IMRT (full course) | ₹1,20,000 – ₹2,50,000 | 60–70 Gy over 6–7 weeks |
| Concurrent Chemoradiation (CCRT) | ₹1,80,000 – ₹3,50,000 | Radiation + weekly cisplatin; 7-week course |
| Pembrolizumab (per cycle) | ₹2,00,000 – ₹2,50,000 | For recurrent / metastatic OSCC; insurance coverage varies |
| Full Multi-modal Treatment | ₹1,50,000 – ₹12,00,000+ | Depending on stage, reconstruction, and systemic therapy |
Costs are indicative. A personalised treatment cost estimate is provided following your initial oncology consultation at CION.
CION Cancer Clinics is India's fastest-growing cancer care network, with over 35 centres across Telangana and Andhra Pradesh. Dedicated exclusively to oncology, CION delivers NABH-accredited, NCCN and ESMO protocol-driven cancer care — bringing world-class treatment closer to patients across the region.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.
Microvascular free-flap reconstruction is the gold standard for restoring oral form and function after wide resection — yet no other hospital treatment page in Hyderabad currently explains it. CION coordinates radial forearm, fibula, and ALT free flaps as part of oral cancer surgical planning, with reconstruction planning that begins before surgery.
From early-stage oral lesions to advanced head-and-neck reconstruction — the people behind our 4.8 / 5 rating across 1,000+ Google reviews.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
























Read all 800+ reviews on Google
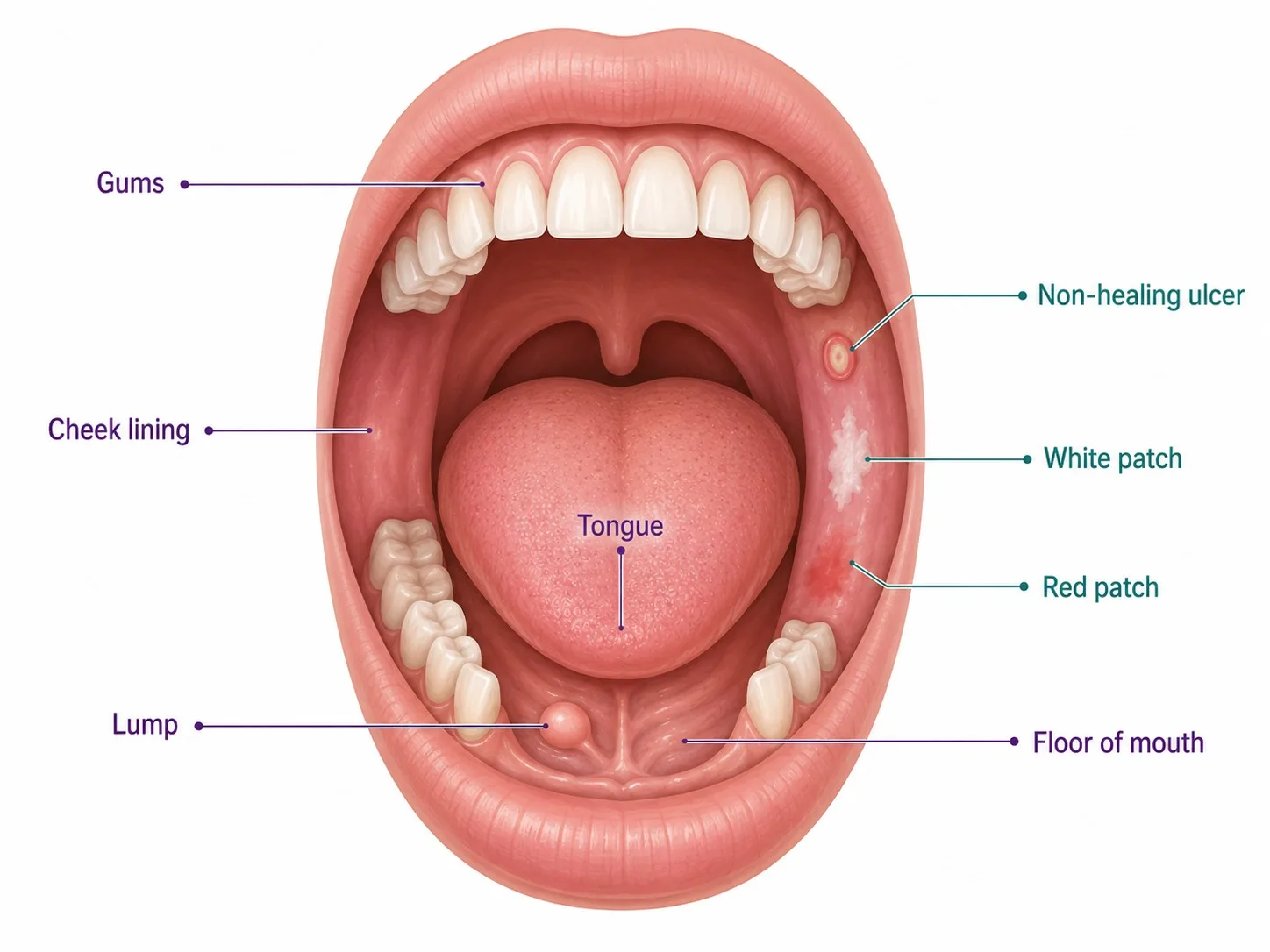
Start Your Story. Book Free Consultation.The most important warning sign is a mouth ulcer or sore that has not healed within 3 weeks — this should always prompt specialist evaluation. Other key symptoms include: a white patch (leukoplakia) or red patch (erythroplakia) anywhere in the mouth; a painless lump or thickening in the mouth or cheek; a lump or swelling in the neck (enlarged lymph node); difficulty or pain on chewing or swallowing; unexplained mouth bleeding; numbness in the tongue or lips; and restricted mouth opening (trismus — particularly in gutka or areca nut users with oral submucous fibrosis). Pain is often absent in early oral cancer — do not wait for pain to develop before seeking evaluation.
Oral cancer treatment costs in Hyderabad vary significantly by stage and extent of surgery. Wide local excision with neck dissection costs approximately ₹1,50,000 to ₹4,00,000. Resection with free-flap reconstruction ranges from ₹4,00,000 to ₹8,00,000. Jaw resection with fibula free flap can reach ₹6,00,000 to ₹12,00,000. Concurrent chemoradiation costs ₹1,80,000 to ₹3,50,000. Pembrolizumab for recurrent/metastatic disease costs ₹1,00,000 to ₹2,50,000 per cycle and may be partially covered by health insurance. CION provides a personalised cost estimate after your initial consultation. EMI payment options are available for all patients.
Yes — oral cancer has among the best cure rates of all head and neck cancers when detected early. Stage I oral cancer has a 5-year survival rate of 80–90% with surgery alone. Stage II achieves 65–80% with surgery and selective adjuvant radiation. Even Stage III disease is curable in many patients with surgery and adjuvant chemoradiation. The most important factor is early detection — oral cancer is almost always visible and accessible during routine self-examination or dental check-ups. If you use tobacco or areca nut in any form, have your mouth examined by a specialist every 6–12 months.
Oral cancer is staged using the AJCC TNM system (8th edition). Stage I: tumour ≤2cm, no lymph node involvement, no spread — 5-year survival 80–90%. Stage II: tumour 2–4cm, no nodes — 65–80% survival. Stage III: tumour >4cm or spread to a single ipsilateral lymph node ≤3cm — 40–60% survival. Stage IVA: moderately advanced local or regional disease — 25–40% survival. Stage IVB/C: very advanced local disease or distant metastases — 10–20% survival. Stage at diagnosis is the primary determinant of treatment approach and outcome; this is why prompt evaluation of any oral warning sign is critical.
The overwhelming cause of oral cancer in India — and particularly in Telangana and Andhra Pradesh — is tobacco in its many forms: gutka, pan masala, khaini (smokeless tobacco forms placed in the cheek or lip), cigarettes, and bidis. Areca nut (supari) chewing — even without tobacco — is classified as a Group 1 carcinogen by the WHO and causes oral submucous fibrosis, which carries a significant risk of progressing to oral cancer. Alcohol consumption synergistically multiplies tobacco's carcinogenic effect. HPV-16 infection is an additional risk factor particularly for oropharyngeal cancer. India accounts for approximately 30% of the world's oral cancer burden — almost entirely because of tobacco use.
Overall 5-year survival rates for oral cavity cancers in India range from approximately 40–60% across all stages combined — lower than in Western countries primarily because the majority of Indian patients are diagnosed at Stage III or IV. Stage-specific survival is much better: Stage I achieves 80–90%, Stage II 65–80%. The survival gap is a detection gap — patients who present early because they know the warning signs and do not delay consultation have dramatically better outcomes. Access to care at a specialist oncology centre with reconstructive capabilities and immunotherapy further improves survival in advanced disease.
Yes, in specific situations. For locally advanced unresectable oral or oropharyngeal cancer, definitive concurrent chemoradiation (CCRT) — radiation therapy with simultaneous cisplatin or cetuximab chemotherapy — can achieve local control and cure without surgery. For patients with early-stage superficial lesions on the tongue or floor of mouth, transoral laser microsurgery offers a minimally invasive surgical alternative with excellent functional outcomes. For recurrent or metastatic disease not amenable to further surgery or radiation, pembrolizumab-based immunotherapy and systemic chemotherapy are the primary treatments. CION's tumour board evaluates every patient for all treatment options before recommending surgery.
Neck dissection is the systematic surgical removal of lymph nodes in the neck, performed alongside oral tumour resection. The cervical (neck) lymph nodes are the first site of spread for oral cavity cancers — approximately 30% of patients have microscopic lymph node involvement even when nodes feel normal on examination. Neck dissection serves two purposes: it removes clinically evident lymph node metastases (therapeutic dissection), and it removes at-risk lymph nodes even when they appear normal (elective dissection) to prevent future neck recurrence. Types include selective neck dissection, modified radical, and radical neck dissection. CION performs neck dissection as a standard component of most oral cancer surgeries.
Reconstructive surgery restores the form and function of the mouth after tumour removal. For small defects, primary closure or local tissue rearrangement is possible. For medium defects, a pedicled flap — tissue from the chest or neck — can be rotated to cover the defect. For large defects — particularly after partial tongue removal, floor-of-mouth resection, or jaw resection — microvascular free-flap reconstruction is the gold standard. This involves transferring tissue from a distant donor site (the forearm, thigh, or leg) with its own blood supply, which is reconnected under a microscope. The radial forearm free flap restores tongue and cheek mobility; the fibula free flap replaces jawbone after mandibulectomy. The goal is to restore the patient's ability to eat, speak, and maintain quality of life.
Absolutely — and for oral cancer, it is strongly advisable, particularly for decisions involving jaw resection, free-flap reconstruction, or definitive chemoradiation versus surgery. CION offers a dedicated Second Opinion service where our multidisciplinary tumour board reviews your biopsy, imaging, and existing treatment recommendation. Key situations where a second opinion is especially valuable: when jaw (mandible) removal has been recommended — bone-sparing marginal mandibulectomy may sometimes be an option; when free-flap reconstruction is needed — the choice of flap significantly impacts functional outcomes; and when surgery has been declined as 'not feasible' — CCRT may offer an alternative curative pathway.
Browse our complete guide to oral cancer — types, symptoms, causes, tests and treatment. Tap any topic to read more.