Hyderabad's Multidisciplinary Thyroid Cancer Team
Thyroid Cancer Treatment in Hyderabad — Expert Care Across 7 Locations
Thyroid cancer is the most survivable of all cancers — most people diagnosed with the common papillary and follicular types go on to live completely normal lives after treatment. At CION Cancer Clinics, our team has treated over 1,000 thyroid cancer cases every year across 7 Hyderabad locations, backed by NCCN protocol adherence and NABH-accredited cancer care.
- Thyroidectomy with IONM — nerve-monitoring surgery to protect the voice during thyroid removal
- Radioactive Iodine Therapy — targeted I-131 treatment for papillary and follicular thyroid cancer
- Targeted Therapy — lenvatinib, sorafenib, dabrafenib + trametinib for advanced and refractory cases
- Multidisciplinary Tumour Board — every case reviewed by surgical and medical oncologists together
17+
Cancer Specialists
on Panel
on Panel
96.9%
Breast Cancer
Survival Rate*
Survival Rate*
15,000+
Patients
Treated
Treated
4.8★
Google Rating
(800+ reviews)
(800+ reviews)
Thyroid Cancer in Hyderabad — What You Need to Know
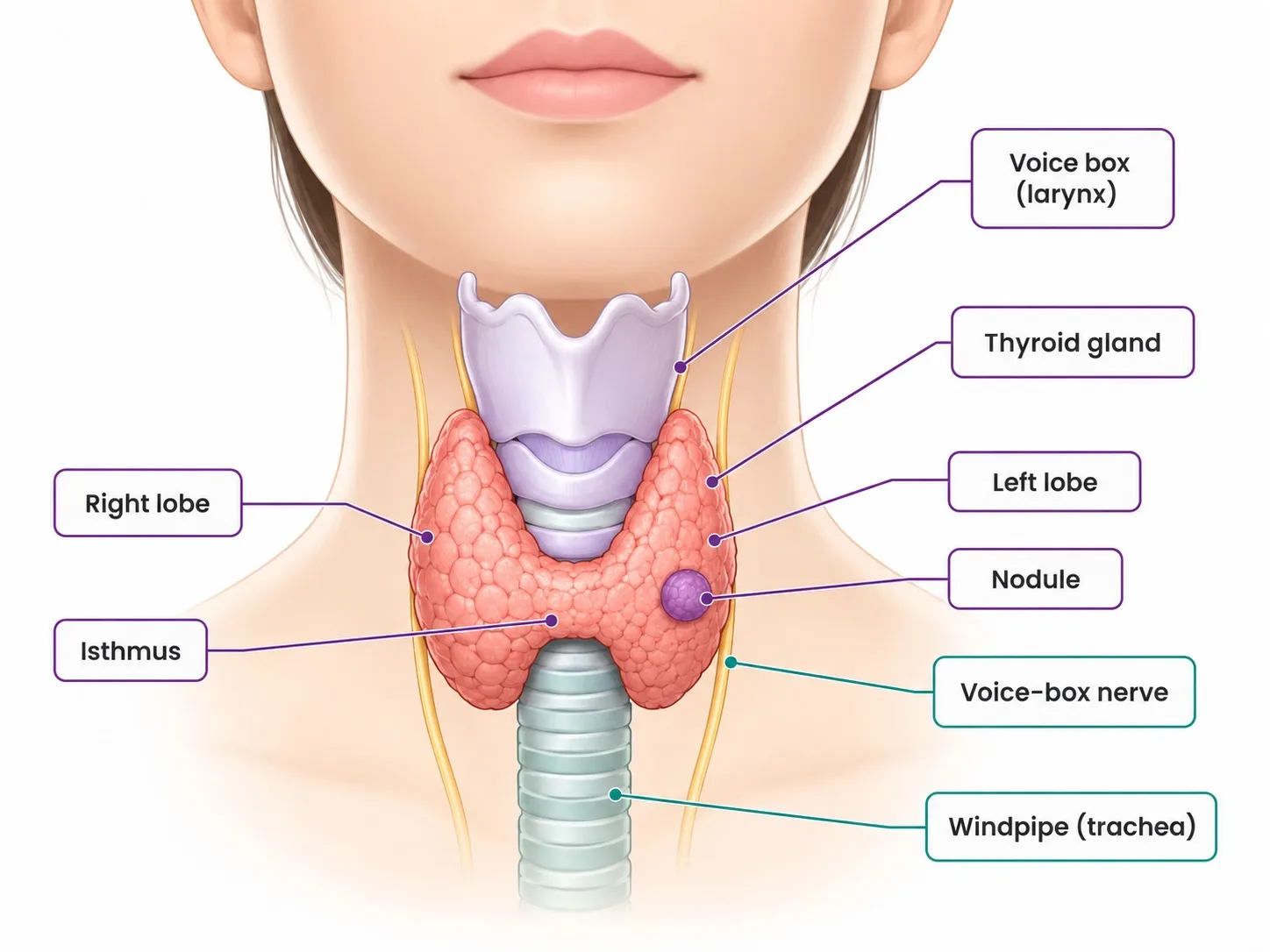
The thyroid is a small, butterfly-shaped gland at the base of your neck that produces hormones controlling how your body uses energy. Thyroid cancer happens when cells in the thyroid gland start growing abnormally. It is more common in women than men — roughly three times more so — and most often diagnosed between the ages of 25 and 65.
The reassuring truth is that most thyroid cancers grow very slowly and are caught early — often during a routine neck ultrasound or checkup for an unrelated condition. Unlike many other cancers, even thyroid cancer that has spread to nearby lymph nodes is often still completely treatable.
The key to the best outcome is specialist oncology care that selects the right treatment for your specific type of thyroid cancer — because different types behave very differently and require entirely different approaches.
Did You Know? Papillary thyroid cancer — the most common type — has a five-year survival rate of over 99% when diagnosed at an early stage. This makes thyroid cancer one of the most treatable cancers in all of oncology. A thyroid cancer diagnosis is scary, but for most people it is very far from a death sentence.
Types of Thyroid Cancer We Treat
There are four main types of thyroid cancer, and each one behaves differently. Knowing your type is the first step to understanding your treatment options.
Papillary Thyroid Cancer — The Most Common and Most Treatable
~80% of cases
About 80% of all thyroid cancers are papillary. It grows very slowly and, even when it spreads to nearby lymph nodes in the neck, it is almost always completely curable with surgery and radioactive iodine treatment. Most people with papillary thyroid cancer live entirely normal lives after treatment with no lasting effects.
Follicular Thyroid Cancer — Also Highly Treatable
~10–15% of cases
Follicular thyroid cancer makes up about 10–15% of cases. It also grows slowly but has a slightly higher tendency to spread through the bloodstream to distant organs like the lungs or bones. When this happens, it still often responds well to radioactive iodine treatment. Detected early, it is highly curable.
Medullary Thyroid Cancer — Rarer, Requires Different Treatment
~5% of cases
Medullary thyroid cancer (MTC) accounts for about 5% of cases. It is different from papillary and follicular cancer in an important way: it does not respond to radioactive iodine, so surgery must remove all the cancer completely. About one in four people with medullary thyroid cancer have inherited it through their family — which is why every patient diagnosed with MTC should be offered genetic testing. If a family gene is found, close relatives can be tested and monitored before cancer even develops.
For medullary thyroid cancer that has spread and cannot be removed with surgery, targeted therapy tablets — vandetanib or cabozantinib — can slow the cancer's growth significantly.
Anaplastic Thyroid Cancer — Rare but Rapidly Growing
<2% of cases · most aggressive
Anaplastic thyroid cancer accounts for less than 2% of thyroid cancers, but it is the most aggressive type — growing and spreading quickly. It requires immediate, intensive treatment combining surgery, radiation, and chemotherapy. However, there is now a genuinely new option for some patients: if the tumour carries a specific genetic change (called BRAF V600E), a combination of two targeted therapy tablets — dabrafenib and trametinib — can dramatically shrink the tumour and significantly improve outcomes, even enabling surgery in some patients who were previously told it was not possible. All patients diagnosed with anaplastic thyroid cancer at CION are tested for this genetic change as standard.
What Increases the Risk of Thyroid Cancer?
Knowing your personal risk helps decide whether a routine neck ultrasound is worth doing as part of a regular check-up.
- Previous radiation treatment to the head or neck — particularly in childhood (for tonsils, acne, or other childhood cancers)
- Family history of thyroid cancer — especially medullary thyroid cancer, which is frequently inherited
- Female gender — women are three times more likely to develop thyroid cancer than men
- Age between 25 and 65 years — though thyroid cancer can occur at any age
- Iodine deficiency — historically relevant in some regions of Telangana and Andhra Pradesh
- Certain inherited conditions — including multiple endocrine neoplasia type 2 (MEN2), familial adenomatous polyposis (FAP), and Cowden syndrome
If you have any of these risk factors, a neck ultrasound is a quick and painless way to check the thyroid before symptoms appear.
Signs and Symptoms of Thyroid Cancer
Thyroid cancer often causes no symptoms at all in its early stages — many cases are found incidentally during an ultrasound done for another reason. To understand the bigger picture, you can watch a Mayo Clinic specialist explain thyroid cancer symptoms and treatment. When symptoms do appear, they may include:
- A painless lump or swelling in the front of the neck — the most common sign; may be the thyroid itself or a lymph node
- A change in your voice — hoarseness or a voice that has become noticeably different, which may indicate the cancer is pressing on the nerve that controls the vocal cords
- Difficulty swallowing — a feeling of something being stuck, or food going down slowly
- Persistent cough — not caused by a cold or throat infection
- Pain in the front of the neck or throat
- Swollen lymph nodes in the neck — usually painless
If you have noticed a lump in your neck — even if it is painless — it is worth getting it checked. Most neck lumps are benign, but a simple ultrasound can confirm this quickly and put your mind at ease. Speak to a CION thyroid cancer specialist if you have symptoms or known risk factors.
12+ Centres in Hyderabad · Pick yours
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centre
Beyond Hyderabad
35+ centres across Telangana & Andhra Pradesh
Travelling for treatment? We may have a centre right where you are.
Telangana
Andhra Pradesh
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Meet the Specialists
17+ senior cancer specialists. One panel for your case.
Trained at AIIMS, Tata Memorial, and leading international centres. Combined 150+ years of experience. Every complex case is reviewed by 3+ of them — together.

Medical Oncologist

Medical Oncologist
Dr. C. Raghavendra Reddy
MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

Medical Oncologist
Dr. Bharati Devi Gorantla
MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

Medical Oncologist
Dr. Owais Mohammed
MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)

Medical Oncologist

Medical Oncologist

Surgical Oncologist
Dr. Muralidhar Muddusetty
MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)

Surgical Oncologist

Surgical Oncologist

Surgical Oncologist
Dr. Vinay Mamidala
MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)

Surgical Oncologist

Radiation Oncologist

Radiation Oncologist

Radiation Oncologist

Hematologist

Interventional Radiologist
Dr. Mohammed Imran

Surgical Oncologist
Dr. Vajja Sandeep Kumar
MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Surgical Oncologist
Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationBook an appointment with our specialist
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Your Treatment Plan, Reviewed by a Team — Not One Doctor's Opinion
Every CION thyroid cancer case goes through our multidisciplinary tumour board — surgical and medical oncologists together — before any treatment begins.
How Is Thyroid Cancer Diagnosed at CION?
Thyroid cancer diagnosis is primarily ultrasound and biopsy driven. CION's diagnostic pathway is designed to reach a clear answer efficiently — and to avoid unnecessary tests.
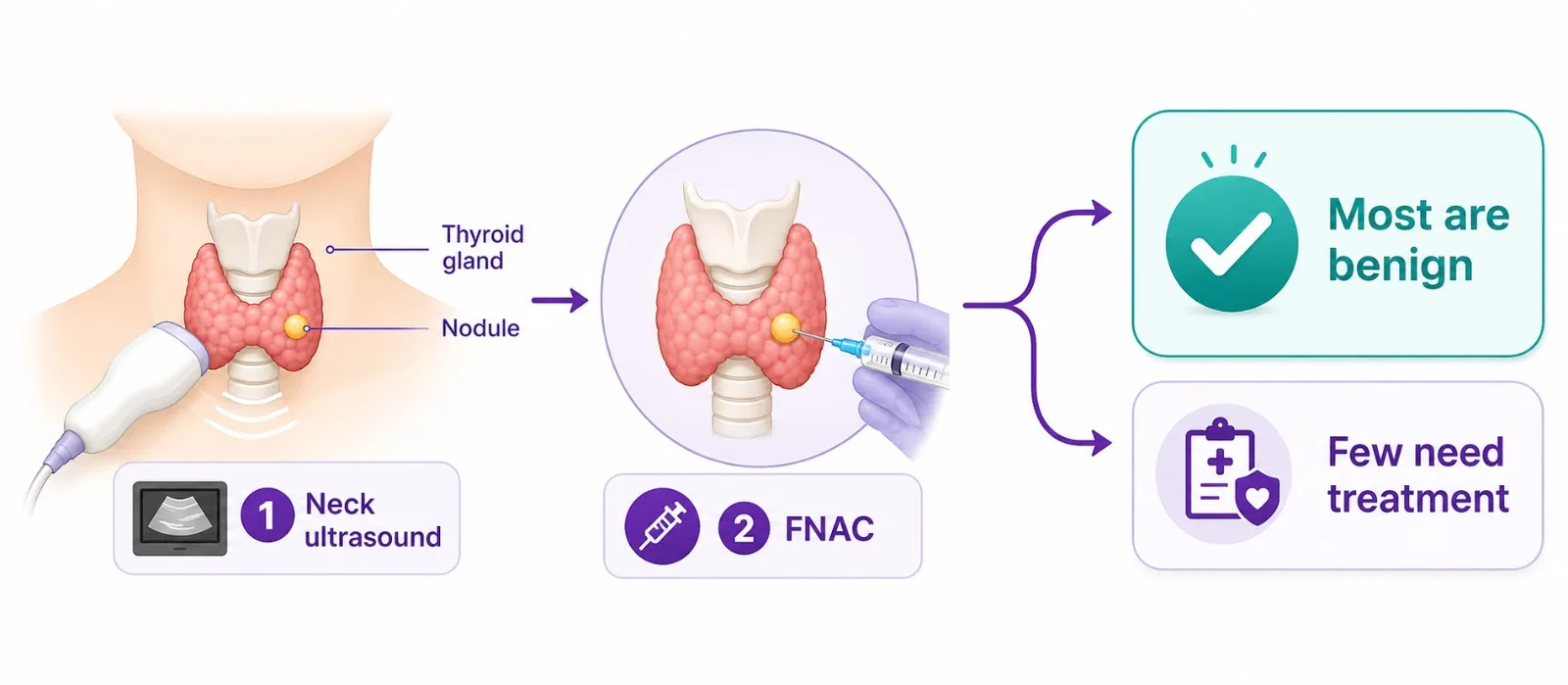
Neck Ultrasound
The first and most important investigation for any suspicious thyroid lump. Quick, painless, and uses sound waves to create a detailed picture of the thyroid gland and nearby lymph nodes. The appearance of a nodule on ultrasound — its size, shape, and characteristics — tells the doctor how likely it is to be cancerous before any other tests are done.
Fine Needle Aspiration Cytology (FNAC)
If a nodule looks suspicious on ultrasound, a very thin needle is used to take a tiny sample of cells from it — guided by the ultrasound to make sure the right spot is sampled. A quick procedure done under local anaesthesia, similar to a blood test, and the sample is examined under a microscope to confirm whether cancer cells are present.
Blood Tests
Thyroid function tests (TSH, T3, T4) check how well the thyroid is working. Thyroglobulin (Tg) is a protein made by the thyroid and used as a tumour marker after treatment. Calcitonin is specifically elevated in medullary thyroid cancer and is tested in all suspected or confirmed MTC cases. CEA is another marker used in medullary thyroid cancer monitoring.
Imaging for Staging
CT scan (neck and chest) assesses whether cancer has spread to lymph nodes or lungs. MRI is used when local invasion of nearby structures (trachea, oesophagus, large blood vessels) is suspected. Whole-body radioiodine scan is performed after surgery to detect any remaining thyroid tissue or cancer cells that have spread, and to plan radioactive iodine treatment.
Thyroid Cancer Staging and Survival Rates
Thyroid cancer is staged differently from most cancers — age at diagnosis matters significantly for papillary and follicular types, and the staging system was updated in 2017 to reflect how well-behaved most differentiated thyroid cancers are. The table below gives a general guide.
| Stage | Cancer Status | What This Means | 5-Year Survival | Typical Treatment |
|---|---|---|---|---|
| Stage I | Confined to thyroid; patient under 55 | Cancer is in the thyroid only | >99% | Surgery ± radioactive iodine |
| Stage II | Spread to nearby tissue; under 55 OR older with small tumour only | Cancer may have spread to nearby lymph nodes or tissue | 95–99% | Surgery + radioactive iodine + hormone tablets |
| Stage III | More extensive local spread in older patients | Cancer has grown into nearby neck structures or lymph nodes | 75–90% | Surgery + radioactive iodine + targeted therapy if needed |
| Stage IV | Spread to distant organs (lungs, bone) OR anaplastic cancer | Cancer has spread beyond the neck area | Varies widely by type | Targeted therapy ± surgery, radiation; anaplastic: intensive multimodal |
Survival rates are for papillary and follicular thyroid cancer treated at specialist oncology centres. Medullary and anaplastic thyroid cancers have different survival profiles; individual outcomes depend on age, cancer type, and response to treatment.
Thyroid Cancer Treatment at CION Cancer Clinics
The right treatment depends on your type of thyroid cancer, how far it has grown, your age, and your overall health. Every patient's case at CION is reviewed by our multidisciplinary team before a treatment plan is finalised.
Surgery — Removing the Thyroid
Surgery is the main treatment for most thyroid cancers. CION's surgical oncology team performs thyroid surgery with a focus on two priorities: removing the cancer completely, and protecting the structures around the thyroid — particularly the nerve that controls the voice and the small glands behind the thyroid that regulate calcium levels.
- Total Thyroidectomy — the entire thyroid gland is removed; used for most papillary and follicular cancers above 1cm, all medullary thyroid cancers, and anaplastic thyroid cancers; after surgery, patients take a daily thyroid hormone tablet (levothyroxine) for life
- Lobectomy — only the half of the thyroid containing the cancer is removed; suitable for small, low-risk papillary cancers confined to one lobe; the remaining thyroid tissue can continue producing hormones, so some patients do not need lifelong hormone tablets
- Neck Dissection — if the cancer has spread to lymph nodes in the neck, these are removed at the same time as the thyroid
Protecting Your Voice During Thyroid Surgery — IONM
One of the biggest concerns people have before thyroid surgery is: will my voice change? This is a valid worry — the nerve that controls the vocal cords (the recurrent laryngeal nerve) runs directly alongside the thyroid gland, and if it is damaged during surgery, it can cause hoarseness or voice change.
At CION, we use intraoperative nerve monitoring (IONM) during thyroidectomy. This means a small probe continuously checks the nerve's function throughout the operation — in real time. If the surgeon gets too close to the nerve, the monitor gives an immediate alert. This technology significantly reduces the risk of voice change after surgery and gives patients reassurance that every precaution is being taken to protect their vocal cords.
Temporary hoarseness after thyroid surgery is possible and usually resolves within a few weeks. Permanent voice change is uncommon at experienced centres using IONM.
Radioactive Iodine (RAI) — The Thyroid's Unique Treatment
After surgery, most people with papillary or follicular thyroid cancer receive radioactive iodine treatment — often called RAI or I-131. This is one of the most targeted cancer treatments in all of medicine, because the thyroid is virtually the only tissue in the body that absorbs iodine.
Here is how it works: you swallow a capsule or drink containing radioactive iodine. It travels through your bloodstream and is absorbed only by thyroid tissue — including any remaining cancer cells that may have spread to lymph nodes or the lungs. The radioactivity then destroys these cells from the inside, while the rest of your body is largely unaffected. The treatment is done as an inpatient stay of 1–2 days, after which the radioactivity leaves your body naturally through urine.
Preparing for Radioactive Iodine — What You Need to Know
For RAI to work effectively, your thyroid cells need to be as hungry for iodine as possible. There are two practical steps that help achieve this:
Low-Iodine Diet (2 Weeks Before Treatment)
For about two weeks before your RAI treatment, you will be asked to follow a low-iodine diet (LID). This means avoiding foods high in iodine — particularly iodised salt and any foods made with it, seafood (fish, prawns, crab, lobster, seaweed), dairy products (milk, curd, paneer, cheese, butter), eggs (particularly egg yolk), commercial baked goods made with iodate dough conditioners, and soya products and some red food dyes. By reducing iodine intake, your remaining thyroid cells become starved of iodine and absorb the radioactive dose more aggressively — making the treatment more effective. Your CION care team will provide a detailed diet guide before treatment.
Raising TSH Levels
Thyroid cells absorb iodine better when stimulated by a hormone called TSH (thyroid-stimulating hormone). Before RAI, your TSH levels are raised either by temporarily stopping your thyroid hormone tablet (thyroid hormone withdrawal) or by an injection of a synthetic version of TSH (rhTSH injection). Your doctor will discuss which approach is right for you.
TSH Suppression Hormone Therapy — Tablets for Life
After surgery and RAI, virtually all thyroid cancer patients take a daily thyroid hormone tablet — levothyroxine. This does two things: it replaces the hormones your removed thyroid can no longer produce, and in higher doses, it suppresses TSH (thyroid-stimulating hormone), which can stimulate any remaining cancer cells to grow. The dose is carefully adjusted based on your cancer risk — patients with higher-risk cancers have their TSH kept lower; lower-risk patients can have a dose closer to normal. Your dose will be reviewed regularly with blood tests.
When RAI Stops Working — What Happens Next
In a small number of patients with papillary or follicular thyroid cancer — roughly 5–15% — the cancer eventually stops responding to radioactive iodine. This happens because the cancer cells change over time and lose their ability to absorb iodine. When this occurs, it does not mean all options are exhausted.
For patients whose cancer is growing and no longer responds to RAI, targeted therapy tablets are the next step. These are daily oral medications — lenvatinib or sorafenib — that work by cutting off the blood supply that tumours need to grow. They are not a cure, but clinical studies have shown they can stabilise the cancer for months or years. Side effects include high blood pressure, fatigue, and appetite changes, which are monitored and managed throughout treatment.
For medullary thyroid cancer that has spread, similar targeted therapy tablets — vandetanib or cabozantinib — are used. These drugs specifically target the pathway that medullary thyroid cancer relies on to grow.
If you have been told your thyroid cancer is no longer responding to radioactive iodine and you have not been offered targeted therapy, request a review by CION's oncology team.
Did You Know? About 25% of medullary thyroid cancers are caused by an inherited gene change that can affect other family members. A simple blood test (genetic testing) can identify this gene. If found in your family, close relatives can be monitored — or even have preventive surgery — before cancer develops. This is why genetic testing is offered to every medullary thyroid cancer patient at CION.
Medullary Thyroid Cancer — What It Means for Your Family
About 25% of medullary thyroid cancer cases are caused by an inherited gene change that runs in families. The gene involved is called RET. If you carry this change, your children, siblings, and parents have a 50% chance of carrying it too — and if they do, they may develop medullary thyroid cancer later in life.
This is why genetic testing is offered to every patient diagnosed with medullary thyroid cancer at CION — not just those with a family history. The test is a simple blood test. If the gene change is found, your close family members can be tested too. Family members who carry the gene can be monitored closely, and in some cases, preventive surgery can remove the thyroid before cancer ever develops.
This family-protection aspect of medullary thyroid cancer management could genuinely save lives among your family members. If you have been diagnosed with medullary thyroid cancer and not offered genetic testing, please ask for it at your next appointment.
Do You Always Need Surgery for Thyroid Cancer?
Many people are surprised to hear that for very small, very slow-growing thyroid cancers — specifically papillary thyroid microcarcinomas under 1cm that have no concerning features — surgery is not always the immediate answer.
For carefully selected patients, NCCN guidelines now endorse an approach called active surveillance: the cancer is monitored closely with regular ultrasound checks (every 6–12 months) instead of proceeding straight to surgery. If the cancer starts growing or shows any concerning changes, surgery is then recommended. If it stays stable — which it very often does — the patient avoids the risks and lifelong hormone tablet requirements of surgery.
Active surveillance is not appropriate for everyone — it depends on the tumour's characteristics, location, your age, and your preference. But if you have been told you have a very small thyroid cancer and are anxious about whether you need surgery right away, this is a conversation worth having with your CION oncologist. You may have more time and more choices than you realise.
External Beam Radiation Therapy
Standard radiation therapy plays a limited role in most thyroid cancers. It is used in specific situations:
- Anaplastic thyroid cancer — radiation is given alongside chemotherapy as part of intensive multimodal treatment
- Medullary or differentiated thyroid cancer that cannot be removed with surgery and does not respond to RAI
- Palliation — for bone metastases causing pain or spinal cord compression
Life After Treatment — Staying Cancer-Free
Thyroid cancer has one of the best long-term outlooks of any cancer — but regular follow-up is important to catch any recurrence early, when it is most treatable.
- Thyroglobulin blood test — after total thyroidectomy, thyroglobulin (a protein made only by thyroid tissue) should be undetectable. Rising thyroglobulin levels can be the earliest sign of recurrence, often before anything shows on a scan
- Neck ultrasound — usually done every 6–12 months for the first few years after treatment, then less frequently as time passes
- Levothyroxine dose monitoring — regular TSH blood tests to ensure your hormone levels are in the right range for your risk category
- Whole-body RAI scan — performed in selected higher-risk patients after surgery to check for any distant spread
- CT or MRI — if blood tests or ultrasound suggest recurrence
Most thyroid cancer patients live completely normal lives after treatment. The follow-up appointments are a routine part of staying well — not a sign that something is wrong.
Multidisciplinary Team — Every Patient's Case Reviewed Together
At CION, your thyroid cancer treatment is never decided by one doctor working alone. Every case is reviewed by a multidisciplinary team — including surgical oncologists, medical oncologists, and where needed, endocrinologists — before any recommendation is made. This means:
- The right choice between total thyroidectomy and lobectomy is made based on your specific tumour
- Active surveillance is considered for eligible low-risk cases, not just surgery by default
- Genetic testing is offered to all medullary thyroid cancer patients at diagnosis
- BRAF V600E testing is arranged for all anaplastic thyroid cancer patients before treatment begins
- RAI preparation guidance — including low-iodine diet instructions — is provided before every RAI treatment
- TSH suppression levels are tailored to your individual risk category
- Targeted therapy is started promptly when RAI stops working
- Long-term surveillance plan is established from day one
- Digital coordination across all 7 Hyderabad locations
Why Patients Choose CION for Thyroid Cancer Treatment in Hyderabad
Eleven reasons our patients pick CION — IONM-protected surgery, NCCN protocols, multidisciplinary review, and full integrative support.
1,000+ thyroid cancer cases
7 locations across Hyderabad
5-Star NABH Accredited
NCCN Protocol Adherence
AIIMS-trained surgical oncologist
Multidisciplinary tumour board
Full integrative support
Dedicated Second Opinion service
EMI facility
4.8 / 5 Google rating
35+ centres across Telangana & AP
Thyroid Cancer Treatment Cost in Hyderabad
Thyroid cancer treatment costs in Hyderabad vary based on the type of cancer, the extent of surgery required, and whether additional treatments such as radioactive iodine or targeted therapy are needed.
| Treatment | Approx. Cost (INR) | Notes |
|---|---|---|
| Lobectomy (Partial Thyroidectomy) | ₹75,000 – ₹2,00,000 | For small, low-risk cancers in one lobe |
| Total Thyroidectomy + Neck Dissection | ₹1,50,000 – ₹3,50,000 | Standard for most papillary, follicular, medullary cases |
| Radioactive Iodine (RAI) Treatment | ₹50,000 – ₹1,50,000 | Includes inpatient isolation stay; dose dependent |
| Levothyroxine (Hormone Tablet) | ₹500 – ₹2,000 / month | Lifelong; regularly monitored with blood tests |
| Targeted Therapy — Lenvatinib / Sorafenib | ₹60,000 – ₹1,80,000 / month | For RAI-refractory disease; insurance coverage varies |
| Targeted Therapy — Dabrafenib + Trametinib | ₹1,00,000 – ₹2,50,000 / month | For BRAF V600E anaplastic thyroid cancer |
| External Beam Radiation (full course) | ₹1,20,000 – ₹2,50,000 | For anaplastic thyroid cancer or palliative cases |
| Full Multi-modal Treatment | ₹1,50,000 – ₹6,00,000+ | Depending on type, stage, and treatment sequence |
Financial Support Options
- EMI Facility — flexible instalment-based payment options available for all patients
- Private Health Insurance — CION works with all major TPAs for cashless hospitalisation; targeted therapy coverage varies by insurer
Costs are indicative. A personalised cost estimate is provided following your initial oncology consultation at CION.
From our patients
Hear From People Who Have Walked This Path
Real stories from thyroid cancer patients treated at CION — from diagnosis to recovery.
Real Stories. Real Voices.
15,000+ patients chose CION. Hear from them directly.
These aren't paid endorsements or written reviews. These are video testimonials from real patients and families — recorded on their own phones, in their own words. Pick any one. Watch it. Then decide.
4.8★800+ Google reviews
50+video testimonials
15,000+patients treated
























Read all 800+ reviews on Google
Start Your Story. Book Free Consultation.Frequently Asked Questions
Common questions about thyroid cancer treatment in Hyderabad — answered by CION's oncology team.
Is thyroid cancer curable?
Yes — thyroid cancer is one of the most curable cancers in oncology. Papillary thyroid cancer, which accounts for 80% of all thyroid cancers, has a five-year survival rate exceeding 99% at early stages. Even when it has spread to nearby lymph nodes in the neck, it is still usually completely curable with surgery and radioactive iodine treatment. Follicular thyroid cancer is similarly treatable. Medullary thyroid cancer requires different treatment (surgery, not radioactive iodine) but is also curable when caught early. Anaplastic thyroid cancer is rarer and more aggressive, but even here, new targeted therapies for patients with a specific gene change have significantly improved outcomes.
What is the cost of thyroid cancer treatment in Hyderabad?
Treatment costs in Hyderabad vary by type and extent of treatment. Lobectomy costs approximately ₹75,000 to ₹2,00,000. Total thyroidectomy with neck dissection ranges from ₹1,50,000 to ₹3,50,000. Radioactive iodine treatment costs ₹50,000 to ₹1,50,000 depending on the dose. Monthly thyroid hormone tablets cost only ₹500–2,000 and are required lifelong. Targeted therapy for advanced cases costs ₹60,000 to ₹2,50,000 per month depending on the drug. CION provides a personalised cost estimate after your initial consultation. EMI payment options are available for all patients.
What is the survival rate for thyroid cancer?
Thyroid cancer has the best overall survival rates of almost any cancer. Papillary and follicular thyroid cancer at Stage I (the most common presentation) have five-year survival rates exceeding 99%. Even at Stage II and III, survival rates remain very high — 95–99% and 75–90% respectively. Stage IV survival varies — for papillary/follicular cancer that has spread to distant organs it is lower, but many patients live for many years on targeted therapy. Anaplastic thyroid cancer has historically had poor survival, but new targeted therapies for patients with the BRAF V600E gene change have meaningfully improved outcomes.
What is radioactive iodine therapy for thyroid cancer?
Radioactive iodine (RAI) is a remarkably targeted treatment that works because the thyroid is virtually the only tissue in the body that absorbs iodine. After thyroid surgery, you swallow a capsule or drink containing radioactive iodine. It travels through your bloodstream and is taken up only by remaining thyroid cells — including any cancer cells that may have spread to lymph nodes or distant organs. The radioactivity destroys these cells from within, leaving the rest of your body largely unaffected. You stay in hospital for 1–2 days while the radioactivity is at its highest, then return home once it has reduced to a safe level. It is used for papillary and follicular thyroid cancers; medullary and anaplastic cancers do not respond to RAI.
What are the symptoms of thyroid cancer?
Thyroid cancer often causes no symptoms in its early stages — many cases are found incidentally during a neck ultrasound. When symptoms do occur, the most common is a painless lump or swelling at the front of the neck. Other symptoms may include: a change in your voice (hoarseness), difficulty swallowing, a persistent cough not caused by a cold, pain in the front of the neck or throat, and swollen lymph nodes in the neck. A neck lump — even if completely painless — is always worth getting checked with an ultrasound and specialist review.
Can thyroid cancer come back after treatment?
Thyroid cancer can recur, but the recurrence rate for well-treated papillary and follicular cancers is low — and most recurrences are still treatable. This is why long-term follow-up with regular thyroglobulin blood tests and neck ultrasounds is important. A rising thyroglobulin level (a protein made only by thyroid tissue) is often the first sign of recurrence — detected before anything shows on a scan — allowing treatment to begin at the earliest possible stage. Medullary thyroid cancer is monitored with calcitonin levels. With regular monitoring, recurrences are caught early and managed effectively in the vast majority of patients.
What is the difference between total thyroidectomy and lobectomy?
A total thyroidectomy removes the entire thyroid gland. After the surgery, you will take a daily thyroid hormone tablet (levothyroxine) for life to replace the hormones your thyroid used to produce. A lobectomy removes only one half (lobe) of the thyroid — the half containing the cancer — leaving the other half in place. The remaining thyroid tissue can continue producing hormones, so some patients who have a lobectomy do not need lifelong hormone tablets, or need a lower dose. Lobectomy is suitable for small, low-risk papillary cancers confined to one lobe. Total thyroidectomy is used for most other cases, and is always recommended for medullary and anaplastic thyroid cancer.
What is active surveillance for thyroid cancer?
Active surveillance means choosing to monitor a very small, very low-risk thyroid cancer with regular ultrasound checks instead of proceeding immediately to surgery. It is an option endorsed by international guidelines (including NCCN) for carefully selected patients with very small papillary thyroid cancers — specifically, cancers under 1cm that are not near critical structures and show no concerning features on imaging. During active surveillance, your oncologist checks the cancer every 6–12 months. If it shows any growth or change, surgery is then recommended. If it stays stable — which many microcarcinomas do for years — unnecessary surgery and its associated risks and lifelong hormone replacement are avoided. Not everyone is a candidate for active surveillance; your CION oncologist will advise whether it is appropriate for your specific situation.
What is anaplastic thyroid cancer?
Anaplastic thyroid cancer (ATC) is the rarest type of thyroid cancer — less than 2% of cases — but the most aggressive. Unlike papillary and follicular cancers that grow slowly over years, anaplastic cancer grows and spreads rapidly, often within weeks. It requires immediate, intensive treatment combining surgery, radiation, and chemotherapy. However, for patients whose anaplastic thyroid cancer carries a specific gene change called BRAF V600E (found in about 40–50% of ATC cases), a combination of two targeted therapy tablets — dabrafenib and trametinib — has shown dramatic results, including significant tumour shrinkage and improved survival. At CION, all anaplastic thyroid cancer patients are tested for this gene change as a standard part of diagnosis.
Can I get a second opinion before thyroid cancer surgery?
Absolutely — and for thyroid cancer, a second opinion can be particularly valuable in three situations: when you have a very small microcarcinoma and want to know if active surveillance is an option; when total thyroidectomy has been recommended and you want to know if lobectomy might be sufficient for your case; and if you have been diagnosed with anaplastic or medullary thyroid cancer, where access to specialised targeted therapies and genetic testing can significantly affect your outcomes. CION offers a dedicated Second Opinion service where our multidisciplinary team reviews your ultrasound, biopsy results, and existing recommendation before advising on the most appropriate path forward.
Disclaimer: This content is intended for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified oncologist for guidance specific to your medical condition. The information on this page is periodically reviewed and updated by CION's medical team in accordance with current clinical guidelines.
Explore more
Thyroid Cancer Topics
Browse our complete guide to thyroid cancer — types, symptoms, causes, tests, stages and treatment. Tap any topic to read more.
Treatment & Specialist Care
Types of Thyroid Cancer
Symptoms & Warning Signs
Causes & Risk Factors
Tests & Diagnosis
Stages, Survival & Prognosis
Treatment & Procedures
Thyroidectomy Surgery
Thyroid Lobectomy
Neck Dissection
Radioactive Iodine (RAI)
Low-Iodine Diet for RAI
Targeted Therapy
External Beam Radiation
Does It Need Chemotherapy?
Treatment Without Surgery
Active Surveillance
Hormone Replacement & TSH
RAI-Refractory Disease
Anaplastic Cancer Treatment
Treatment Side Effects