Breast cancer surgery · 35+ centres across Telangana & AP
Sentinel Lymph Node Biopsy: Why It Matters in Breast Cancer
A sentinel lymph node biopsy checks the very first lymph node your breast tumour would drain into, to see whether cancer has begun to spread. By sampling just one or a few nodes instead of clearing the whole underarm, it gives an accurate answer while sparing most women the swelling, stiffness and lifelong arm care that full axillary clearance can bring.
★★★★★Rated 4.8/5 · 800+ Google reviews · 15,000+ patients treated
MM
Medically reviewed by Dr. Muralidhar Muddusetty, Senior Surgical Oncologist — MBBS (AIIMS), MS Surgery (AIIMS), DNB Surgical Oncology, MRCS (Edinburgh), CION Cancer Clinics. · Reviewed June 2026
Understanding the procedure
What the sentinel lymph node is & why it is sampled
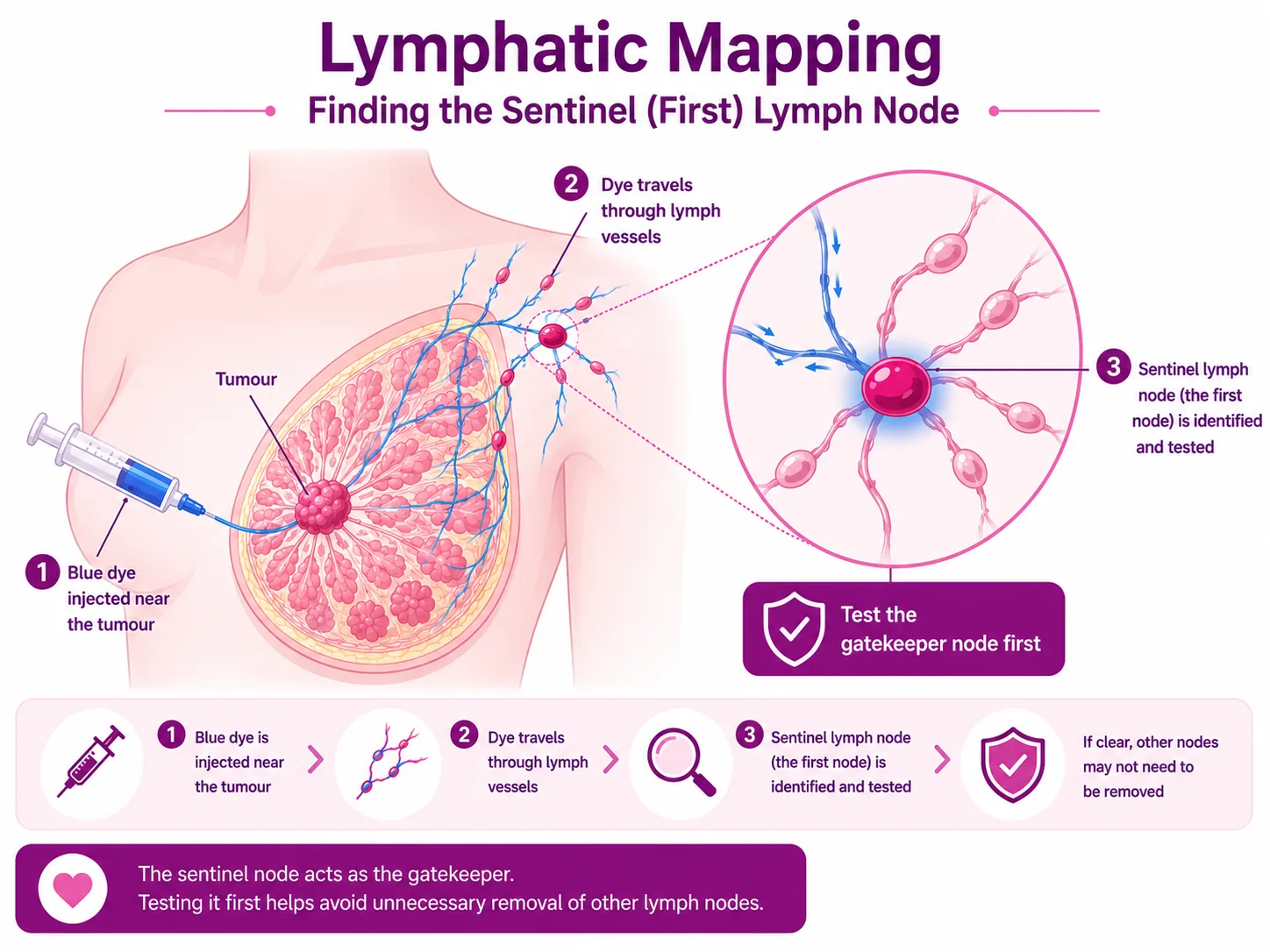
The sentinel node is the first node a breast tumour drains into — usually in the underarm. Because it is first in line, it is where cancer would most likely appear first. Instead of removing every node just to find out, we test the one node that matters most; if it is clear, the nodes beyond it are very likely clear too.
Lymph fluid drains away from the breast in an orderly way. Checking the sentinel node tells us, with high accuracy, whether the cancer has started to spread to the lymph nodes — one of the most important pieces of information for staging and planning treatment.
This matters because the node result changes everything that follows: the stage of the cancer, whether chemotherapy or radiation is advised, and the type of surgery. Imaging and a clinical exam are not enough on their own — a meaningful share of women whose nodes look normal on scans still have microscopic cancer in them. The only reliable way to know is to remove and examine the sentinel node itself. At CION Cancer Clinics, this principle guides how we stage the axilla for early breast cancer.
The sentinel node is the first “gatekeeper” node the tumour drains into — testing it first spares the other underarm nodes.
How it works
How a sentinel node biopsy is done (dye & isotope mapping)
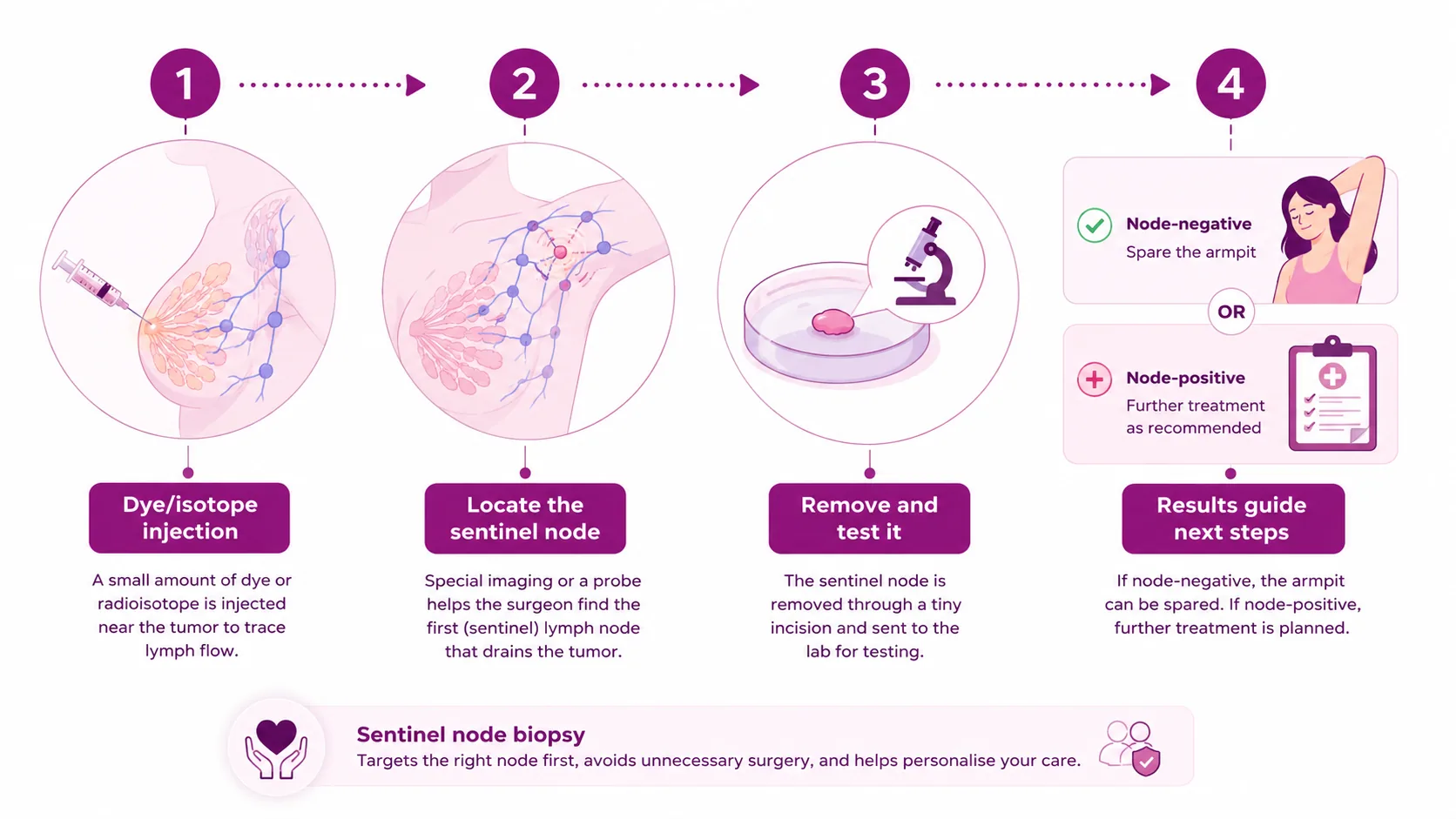
The procedure is built around mapping. A small amount of tracer is injected near the tumour or around the nipple; it travels the exact path lymph fluid would take and marks the first draining node. Guided by a probe or the dye, the surgeon removes one to three marked nodes through a small underarm incision — usually under general anaesthesia, often during the breast surgery itself.
The sentinel node biopsy in four steps — inject and trace, locate, remove and test, then let the result guide the next step.
The tracers surgeons use — often two together for the best accuracy:
Radioactive isotope (technetium-99m)
A small, safe dose injected before surgery and detected with a handheld gamma probe. The radioactivity is very low and clears within a day or two. It is the most established mapping agent.
Blue dye mapping
A blue dye injected near the tumour visibly stains the sentinel node, which the surgeon follows by eye. Inexpensive and widely available in Indian practice — best paired with a second tracer.
ICG fluorescence
Indocyanine green lights up the node under a near-infrared camera in real time — a radiation-free option giving identification rates close to the isotope, without a nuclear-medicine facility.
Dual technique for best accuracy
Combining two tracers raises the chance of finding the true sentinel node to around 98% and lowers the false-negative rate. CION's surgical team favours a dual approach wherever feasible.
Did you know? A large Indian tertiary-centre study found the sentinel node was correctly identified about 98% of the time with the dual dye method versus 94% with blue dye alone, with a false-negative rate under 1%. Source: Tata Medical Center, India (PMC9300403).
Understanding your result
What a positive vs negative sentinel node means
In roughly 70–80% of early breast cancers the sentinel node is negative — reassuring news that usually means no more underarm surgery. A positive result is not a disaster either; it simply guides a well-established next step, decided by your tumor board.
Understand each result
Simplified for understanding. Your exact result and plan are decided by your oncology team after surgery and pathology.
Negative (70–80% of cases)
No cancer in the first node — spread is unlikely, and usually no further node surgery is needed. You avoid a bigger operation and its side effects.
Positive doesn't always mean more surgery
Thanks to the ACOSOG Z0011 evidence, many women with only one or two positive sentinel nodes who are having breast-conserving surgery and radiation can safely skip further node surgery.
Why the change
Why it replaced full axillary clearance (less lymphedema)
Sampling the sentinel node is as safe as clearing the whole axilla for the right patients — with far fewer side effects. Landmark trials, including ACOSOG Z0011, showed the same survival and very low recurrence, but a striking drop in arm swelling: about 0.5–3% after sentinel biopsy versus roughly 5–17% after full axillary dissection.
For decades the standard was axillary lymph node dissection (ALND) — removing most or all of the underarm nodes. It worked, but removing so many nodes disrupts lymph drainage from the arm, causing a real risk of lymphedema (long-term arm swelling), shoulder stiffness, numbness and cording — often lifelong. Today, sentinel node biopsy is the recommended first approach for the right patients, with full clearance reserved for those who genuinely need it.
Much less lymphedema
About 0.5–3% arm-swelling risk after sentinel biopsy versus roughly 5–17% after full axillary clearance.
Same safety, proven by Z0011
For early node-negative cancer, sampling the sentinel node matches full dissection on survival and recurrence.
Less stiffness and numbness
A smaller incision and fewer nodes removed mean less shoulder restriction, cording and nerve disturbance.
After your surgery
Recovery & arm care after a sentinel node biopsy
Recovery is gentle. The incision is small, and most women go home the same day or the next morning. Expect some soreness, bruising and mild underarm swelling for a couple of weeks; if blue dye was used, your skin and urine may be tinted for a day or two — harmless and fades on its own.
Same-day or next-day discharge
The small incision means most women recover at home quickly, with light activity in a few days and a gradual return to exercise over two to three weeks.
Gentle shoulder exercises
Easy, guided shoulder and arm movements within the first days prevent stiffness and cording. CION's physiotherapy team shows you exactly what to do and when to progress.
Protect the arm from injury
Avoid cuts, burns and insect bites on the operated side, keep the skin moisturised, and treat any small wound promptly — minor skin breaks are the commonest trigger for arm swelling.
Watch for and report swelling
Tell your team early if the hand, forearm or upper arm feels heavy, tight or looks larger — early lymphedema is far easier to control, and the overall risk is low to begin with.
Care for the wound
Keep the incision clean and dry as instructed, and contact us for fever, spreading redness, increasing pain or fluid build-up (seroma). These are uncommon and settle quickly when caught early.
Support beyond surgery
Nursing and physiotherapy teams teach arm care before you go home, so movement returns fully and your already-low lymphedema risk stays low.
Am I a candidate?
Could a sentinel node biopsy be right for you?
Sentinel node biopsy is the standard approach for early breast cancer where the underarm nodes look and feel normal (clinically node-negative). It is generally not the first choice when there is already obvious, bulky cancer in the underarm nodes. Whether it suits you depends on your tumour, scans, and overall plan — always decided with your tumor board.
Quick check: might this apply to you?
Tick anything that describes your situation. This is an awareness guide, not a diagnosis or a treatment decision.
This tool doesn't decide your surgery or replace a specialist opinion. Your suitability for a sentinel node biopsy is confirmed by your oncology team after examination and scans.
Cost
Cost of a sentinel node biopsy in Hyderabad
The cost depends on the tracer method, whether it's done with your breast surgery, hospital stay and room category — best given as an indicative range after assessment. Eligible breast cancer treatment may be covered under Aarogyasri / PMJAY at empanelled centres, and we help with insurance and EMI. See our breast cancer treatment cost guide.
What affects the cost
The mapping technique (dye, isotope, ICG or dual), whether the biopsy is combined with your main breast surgery, anaesthesia, pathology and room category.
Scheme & insurance cover
Eligible treatment may be largely covered under Aarogyasri and PMJAY at empanelled centres. Our team helps check eligibility and guides you on insurance and EMI.
A transparent estimate
You get a clear, upfront estimate — including diagnostics — with no unnecessary tests and no hidden charges, before anything is planned.
Ask whether a sentinel node biopsy is right for you — free
Newly diagnosed, or unsure about your underarm surgery plan? Book a free consultation and, if you already have a biopsy, a free written second opinion.
Your case reviewed by a multidisciplinary tumor board
Every option explained with clear, upfront costs
Aarogyasri / PMJAY & insurance guidance
9 clinics in Hyderabad · 35+ across Telangana & AP
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the surgical oncologists
Your breast surgery is planned by a team, not one doctor.
Surgical, medical and radiation oncologists agree your axillary plan together in a multidisciplinary tumor board — part of 17 senior specialists across CION.
Worry and misinformation keep people from the least invasive option. Here are the beliefs we hear most, and the facts.
“Removing the sentinel node will make my cancer spread.”
Fact: Sampling one to three nodes is a safe, standard, controlled step — it does not spread cancer. The real risk is delay, which lets a treatable cancer grow.
“A node biopsy means my cancer is already advanced.”
Fact: It is a staging step, not a verdict. In about 70–80% of early breast cancers the sentinel node comes back negative.
“If the node is positive I'll always lose my whole armpit.”
Fact: Not any more. Thanks to the Z0011 evidence, many women with one or two positive nodes having breast-conserving surgery and radiation safely avoid full clearance.
“Sampling one node isn't as reliable as removing them all.”
Fact: With dual mapping the true sentinel node is found about 98% of the time and the false-negative rate is under 1% — as safe as full clearance for the right patients.
“I'll definitely get lymphedema after node surgery.”
Fact: The risk is low — only about 0.5–3% after a sentinel node biopsy, versus roughly 5–17% after full axillary dissection.
“The blue dye or the radioactive tracer is dangerous.”
Fact: The tracer dose is very low and clears from the body within a day or two; the blue dye harmlessly tints skin and urine for a day or two.
“It's a big operation with a long hospital stay.”
Fact: The incision is small and most women go home the same day or the next morning, often with the biopsy done during the breast surgery itself.
“There's nothing I can do to protect my arm.”
Fact: Simple, lifelong-friendly arm care — protecting the skin, gentle shoulder exercises and reporting swelling early — keeps the already-low risk low.
“A second opinion on my surgery plan will offend my surgeon.”
Fact: Second opinions are normal and welcomed in cancer care — they confirm the plan and give you confidence. At CION it's free when you have a biopsy report.
“Good breast surgery is unaffordable.”
Fact: You get a transparent estimate up front, and eligible treatment may be covered under Aarogyasri, PMJAY or insurance — our team helps you check.
Why CION
Why choose CION for your breast surgery
A dedicated cancer network
CION treats cancer and only cancer — focused, patient-specific care, not a general hospital's approach.
Tumor board for every case
Surgical, medical and radiation oncologists agree your axillary plan together — never one opinion.
Close to home
9 clinics across Hyderabad and 35+ centres across Telangana & AP, so care and follow-up don't mean long journeys.
Affordable & transparent
Indicative costs up front, Aarogyasri and PMJAY support, and help with insurance and EMI.
Least surgery, safest answer
Full clearance is reserved for those who truly need it, sparing most women avoidable side effects.
Support beyond surgery
Physiotherapy, lymphedema care, nutrition and counselling are built into your plan.
A sentinel lymph node biopsy is surgery to find, remove and examine the first lymph node (or few nodes) that a breast tumour would drain into — usually in the underarm. Because it is first in the drainage path, it is where cancer cells would most likely appear first if the cancer had begun to spread. Checking it tells your team, with high accuracy, whether cancer has reached the lymph nodes — a key part of staging. The clever part is that instead of removing every node just to find out, the surgeon tests only the node that matters most. If it is clear, the nodes beyond it are very likely clear too, so most women avoid a much bigger operation.
How is a sentinel node biopsy done?
Before or during surgery, a tracer is injected near the tumour or around the nipple. It travels the same path lymph fluid would, marking the sentinel node so the surgeon can find it. Surgeons use a blue dye, a radioactive isotope, indocyanine green fluorescence, or — ideally — a combination of two of these, because the dual technique finds the right node most reliably (around 98% versus about 94% for dye alone). Guided by a gamma probe or by the dye/fluorescence, the surgeon removes one to three marked nodes through a small underarm incision, usually under general anaesthesia and often during the breast surgery itself. A pathologist then examines the nodes for cancer cells.
Why did sentinel node biopsy replace full axillary clearance?
For decades the standard was axillary lymph node dissection — removing most underarm nodes. It staged the cancer well but disrupted lymph drainage from the arm, causing a real risk of lymphedema (long-term arm swelling), stiffness, numbness and cording. Landmark trials, including ACOSOG Z0011, showed that for many women with early, clinically node-negative breast cancer, sampling just the sentinel node is as safe as full clearance — same survival and very low recurrence — with far fewer side effects. Arm swelling occurs in only about 0.5-3% after sentinel biopsy versus roughly 5-17% after full dissection. That is why sentinel node biopsy is now the recommended first approach, with full clearance kept for those who truly need it.
What does a positive or negative sentinel node mean?
A negative sentinel node — the result in about 70-80% of early breast cancers — means no cancer cells were found in the first draining node, so spread further along the chain is very unlikely and usually no more nodes need to be removed. A positive sentinel node means cancer cells were found, but this no longer automatically means full axillary clearance. Thanks to the Z0011 evidence and later studies, many women with only one or two positive sentinel nodes who are having breast-conserving surgery and radiation can safely avoid further node surgery. When more nodes are involved, completion dissection or axillary radiation may be advised. At CION the next step is always decided by the tumor board, never by a single rule.
Will I get lymphedema after a sentinel node biopsy?
The risk is low — much lower than after full axillary clearance. Lymphedema (lasting arm swelling) occurs in only about 0.5-3% of women after a sentinel node biopsy, compared with roughly 5-17% after axillary lymph node dissection, because far fewer nodes are removed and lymph drainage is largely preserved. You can lower the risk further with simple arm care: protect the operated side from cuts, burns and insect bites, keep the skin moisturised, do the gentle shoulder exercises your physiotherapist teaches, and report any heaviness, tightness or swelling early. Caught early, swelling is far easier to control. CION's nursing and physiotherapy teams guide you through all of this before you go home.
What is recovery like after a sentinel node biopsy?
Recovery is gentle compared with bigger node surgery. The incision is small, and most women go home the same day or the next morning. Expect some soreness, bruising and mild underarm swelling for a couple of weeks; if blue dye was used, your skin and urine may be tinted for a day or two, which is harmless. Most everyday activities return within a few days, with heavier lifting and exercise resumed gradually over two to three weeks. Gentle, guided shoulder exercises help prevent stiffness. Contact your team promptly for fever, spreading redness, increasing pain, or fluid build-up (seroma) — these are uncommon and usually settle quickly when caught early.
Am I a candidate for a sentinel node biopsy?
Sentinel node biopsy is the standard approach for early breast cancer where the underarm nodes look and feel normal (clinically node-negative) on examination and scans. It is generally not the first choice when there is already obvious, bulky cancer in the underarm nodes, where full clearance may be needed instead. Whether it suits you depends on your tumour, your scans, whether you are having chemotherapy before surgery, and your overall plan. At CION, our tumor board reviews these details together and explains clearly whether a sentinel node biopsy, axillary radiation or a fuller dissection is right for your case — so the decision is informed, individualised and made with you.
How do I start, and what does it cost at CION?
Start with a free first consultation — book online or call CION at 1800-202-8726. Your first appointment is an unhurried, 45-minute conversation that reviews your diagnosis and scans and lays out your surgical options clearly. If a sentinel node biopsy is part of your plan, we explain exactly how it will be done, what each result would mean, and the costs involved — including any diagnostics — with a transparent estimate in advance and no unnecessary tests. Every breast cancer case is reviewed by our tumor board, so your surgery plan is genuinely personalised. Whether you are newly diagnosed or seeking a second opinion, the first consultation is free.
Explore
Explore breast cancer care
Our complete guide to breast cancer — surgery, diagnosis, treatment, types, symptoms and recovery. Tap any topic to read more.
Early answers change outcomes. Book a free consultation or second opinion at any of our 9 Hyderabad clinics — part of 35+ centres across Telangana & Andhra Pradesh.
Medical disclaimer: This page is for general information and awareness and does not replace professional medical advice, diagnosis or treatment. Always consult a qualified oncologist. Costs shown are indicative only and not a quotation. Content is periodically reviewed by CION's medical team.