FNAC of the Breast: The Fine-Needle Test, Explained Simply
FNAC — fine-needle aspiration cytology — is a quick, minimally invasive test that uses a very thin needle to draw a few cells from a breast lump so a pathologist can check them under a microscope. It's fast, low-cost, and needs no cuts or stitches. At CION Cancer Clinics in Hyderabad, FNAC is read within a proper triple assessment and reviewed by a tumor board — so you get a clear answer, not just a slide report.
Thin needle — usually no cuts, no stitches, often no anaesthesia
Free first consultation for every cancer patient
Read within a full triple assessment, reviewed by a tumor board
★★★★★Rated 4.8/5 · 800+ Google reviews · 15,000+ patients treated
MI
Written by the CION Cancer Clinics Editorial Team · medically reviewed by Dr. Mohammed Imaduddin, Surgical Oncologist (MBBS, MS, M.Ch Surgical Oncology), CION Cancer Clinics. · Reviewed June 2026
Start here
What is FNAC (fine-needle aspiration cytology)?
FNAC uses a very thin needle — finer than the one used to draw blood — to gently draw out a small sample of cells from a breast lump. Those cells are smeared on a glass slide and examined under a microscope by a cytopathologist. The word cytology means the study of individual cells — which is exactly what FNAC looks at.
The purpose is to find out quickly, and with very little discomfort, whether a breast lump is most likely benign (non-cancerous, such as a fibroadenoma or a cyst), suspicious, or malignant (cancer). Because the needle is so fine, FNAC usually needs no cut, no stitches and often no anaesthetic injection, and you can go home straight away.
FNAC is widely used across Hyderabad because it is fast and inexpensive. But an important principle guides how we use it at CION: FNAC is one part of a triple assessment — read alongside the clinical examination and imaging (ultrasound or mammogram). It gives a strong early signal, but it is interpreted in context, never as a stand-alone verdict.
The question everyone asks
FNAC vs core needle biopsy — the differences, and when each is used
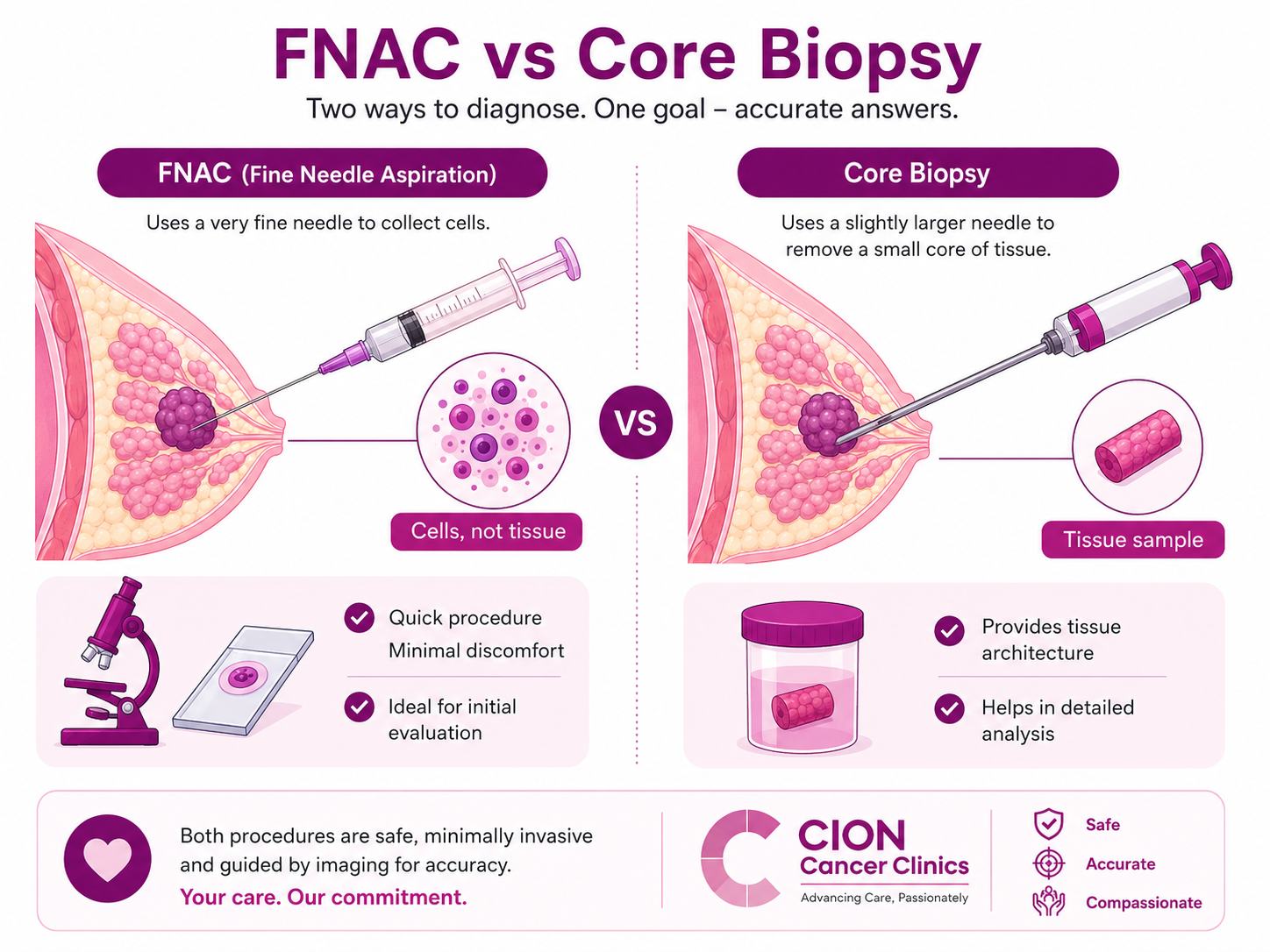
Both sample a breast lump, but they collect different things. FNAC draws out loose cells (cytology). A core needle biopsy removes a tiny core of intact tissue (histology) — which lets the lab tell invasive from in-situ cancer and run the ER, PR and HER2 receptor tests that guide treatment. FNAC cannot reliably do those.
So when is each used? FNAC is fast, very low cost and almost painless, which makes it an excellent first-line check — especially for a lump that looks likely benign, a cyst, or an enlarged underarm lymph node. A core needle biopsy is preferred when cancer is suspected and treatment planning is needed, because it confirms invasive cancer, grades it and runs receptor tests on the same sample.
This choice is made by your specialist after the clinical exam and scan, not by a fixed rule — and sometimes both are used together for the most complete answer.
FNAC collects loose cells; a core biopsy removes a small core of intact tissue.
FNAC is often used first when
The lump is easy to feel, looks likely benign, or for a quick check of a cyst, a lymph node, or a recurrence at a scar — fast, very low cost, and almost painless, ideal for a first-line answer.
Core needle biopsy is preferred when
Cancer is suspected and treatment planning is needed — a core biopsy confirms invasive cancer, grades it, and runs ER, PR and HER2 tests, so guidelines favour it before any cancer surgery or chemotherapy decision.
FNAC came back inadequate or unclear
If a fine-needle sample doesn't have enough cells or the result is borderline, a core needle biopsy is the usual next step rather than repeating FNAC — it minimises the risk of a missed diagnosis.
They can also work together
Studies show the combined accuracy of FNAC plus core biopsy is higher than either alone — the two complement each other, which is why a thorough work-up sometimes uses both.
Step by step
How the FNAC procedure is done
There's no fasting and no injection to prepare for, and the sampling itself takes only a few minutes. If the lump can be felt easily, the doctor may do it by hand; if it's small or deep, an ultrasound-guided FNAC sends the needle exactly to the right spot.
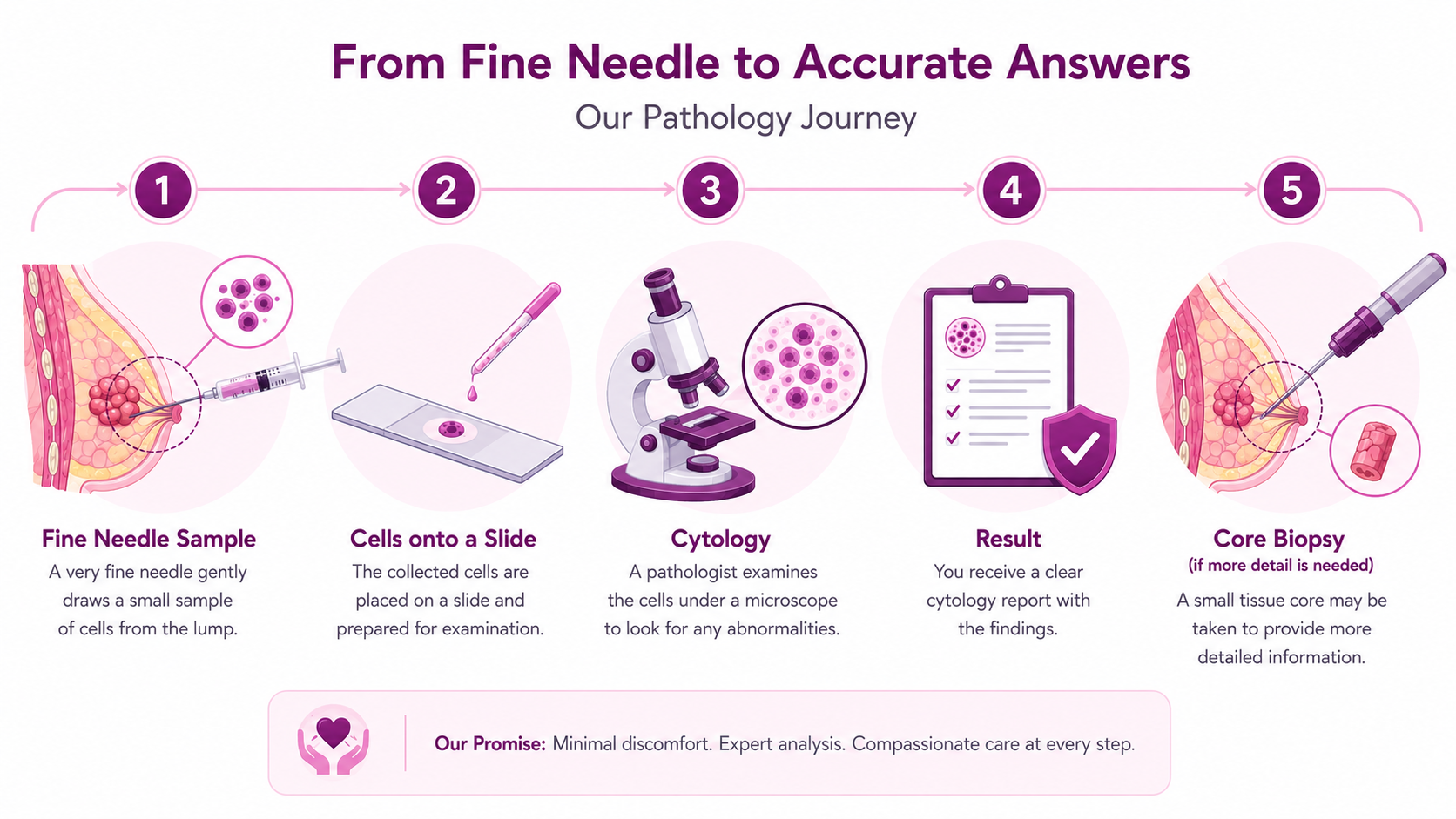
From fine needle to a clear answer — with a core biopsy added only if more detail is needed.
1
Position & clean
You lie or sit comfortably with the arm raised. The skin over the lump is cleaned with antiseptic so the area is sterile before the needle is passed.
2
Locate the lump
The doctor steadies the lump between two fingers. For a small or deep lump, a live ultrasound scan guides the needle precisely — ultrasound-guided FNAC.
3
Aspirate the cells
A very fine needle on a syringe is inserted and moved back and forth a few times to draw a small sample of cells. You may feel a brief pinch or pressure, over in seconds.
4
Prepare the slides
The cells are spread thinly onto glass slides and fixed. A few passes may be taken to make sure there are enough cells for a confident reading.
5
Pressure & home
Light pressure or a small dressing is applied. There are usually no stitches. You return to normal activity the same day; mild bruising settles quickly.
6
Cytopathologist review
A specialist examines the slides under a microscope. At CION the report is read by our specialists and, where needed, taken to the tumor board for full clinical context.
Strengths & limits
What FNAC can — and can't — tell you
FNAC looks at loose cells (cytology); a core biopsy looks at intact tissue (histology). That single difference explains almost everything FNAC can and cannot do — which is why we always read it within a triple assessment.
CAN: confirm a benign cyst or fibroadenoma
When the cells are clearly benign and match a simple cyst or fibroadenoma on the scan and exam, FNAC can give quick, strong reassurance — often saving a more involved biopsy.
CAN: flag malignant cells
A skilled cytopathologist can identify cancer cells with high confidence, giving an early warning that lets your team move quickly to the next, confirmatory step.
CAN: sample lymph nodes & recurrences
FNAC is very useful for checking an enlarged underarm lymph node or a lump at an old surgical scar, where a quick cell sample answers a focused question.
CAN'T: separate invasive from in-situ
With only loose cells and not intact tissue, FNAC can't tell whether a cancer is contained (in-situ, like DCIS) or has begun to invade — a distinction that changes treatment and needs a core biopsy.
CAN'T: reliably run ER, PR & HER2
The receptor tests that decide whether hormone therapy or targeted drugs will help are run on tissue. A core biopsy is needed, so FNAC alone isn't enough to plan cancer treatment.
CAN'T: always grade the cancer
Tumour grade — how aggressive the cancer looks — depends on tissue architecture that FNAC can't fully show, so a core or surgical biopsy is used to grade and stage accurately.
How reliable is it
Accuracy of FNAC — and what happens if it's inconclusive
In a published comparative study of palpable breast lumps, FNAC showed around 74% sensitivity, 77% specificity and 75% overall accuracy, while core needle biopsy reached roughly 85%, 93% and 88%. Combining both raised accuracy to about 88%.* Accuracy depends on the lump's size and location, the number and quality of passes, and the cytopathologist's experience.
Sometimes FNAC comes back inadequate (too few cells) or inconclusive (borderline cells — neither clearly benign nor clearly malignant). This is not a cause for panic; it simply means the test could not give a confident answer. The right response is a calm, structured next step.
If FNAC is benign but doubt remains
When the cells look benign but the exam or scan is still worrying (a "discordant" result), a core needle biopsy is done to be certain — the imaging and clinical picture must agree before we relax.
If FNAC is inadequate
Too few cells means no answer, not a bad one. The usual next step is a core needle biopsy rather than repeating FNAC, since it gives intact tissue and is far less likely to come back inadequate.
If FNAC is suspicious or inconclusive
A borderline result is moved forward, not left hanging — a core biopsy confirms whether cancer is present and, if so, provides the grade and receptor tests needed to plan treatment.
If FNAC confirms cancer
Even a clear malignant FNAC is usually followed by a core biopsy before treatment, because the receptor testing and invasive-versus-in-situ detail it provides are essential to choosing therapy.
*Diagnostic accuracy figures from a comparative FNAC vs core needle biopsy study of palpable breast lumps (PMC9441185, NIH/NCBI). Figures vary between centres and operators.
Book directly
Breast diagnostic services we offer
Everything needed for a complete triple assessment, under one roof — book any of these directly.
FNAC (fine-needle test)
A fine-needle cell sample from a breast lump or lymph node — the fastest, lowest-cost first-line check.
A standard FNAC in Hyderabad typically costs between Rs. 800 and Rs. 2,400, and an ultrasound-guided FNAC around Rs. 2,000 to Rs. 3,500 — depending on the centre, the cytopathologist's expertise, the number of passes, and whether imaging guidance is needed. A core needle biopsy, when required, is priced separately and is modestly higher.
CION runs a network of diagnostic and PET-CT centres across Hyderabad, with up to 50% off on diagnostics for cancer patients and expert-reviewed reporting. Your first consultation is free. Request a callback to book an FNAC, get a cost estimate, or have an existing FNAC or biopsy report reviewed — we'll guide you on whether FNAC, a core biopsy, or both is the right next step.
Standard FNAC
Roughly Rs. 800 to Rs. 2,400 — the lowest-cost way to sample a breast lump.
Ultrasound-guided FNAC
Around Rs. 2,000 to Rs. 3,500 when imaging guidance is needed for a small or deep lump.
Up to 50% off diagnostics
Concessional diagnostic pricing for cancer patients, with expert-reviewed reports.
Insurance & cashless
Cashless private insurance and EMI support available — ask our team for help.
Free consultation
Talk to a breast specialist — free
A worry about a breast lump or an FNAC report shouldn't wait. Book a free consultation and, if you already have a report, a free written second opinion.
Your slides re-read by a senior pathologist
Read within a full triple assessment & tumor board
Up to 50% off diagnostics, with insurance & EMI guidance
9 clinics in Hyderabad · 35+ across Telangana & AP
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Have a breast lump or an FNAC report to review?
Early answers change outcomes. A quick, doctor-led consultation tells you whether you need FNAC, a core biopsy, or simple reassurance — free for your first visit.
Worry and myths keep people away from a simple test. Here are the fears we hear most, and the facts.
“The needle will make the cancer spread.”
Fact: FNAC and biopsies are safe, controlled steps and do not spread cancer. The real risk is delay, which lets a treatable lump grow while you wait.
“FNAC is very painful.”
Fact: The needle is finer than the one used for a blood test. Most people feel only a brief pinch or pressure for a few seconds, and it is often done without any anaesthetic.
“If FNAC is benign, I can forget about it.”
Fact: Usually yes — but if the exam or scan is still worrying, a core biopsy is done to be sure. Benign cytology alone is not the final word when the three checks don't agree.
“FNAC and a biopsy are the same thing.”
Fact: FNAC samples loose cells; a core biopsy removes a small core of intact tissue and can run ER, PR and HER2 tests that FNAC cannot.
“A needle test can confirm my whole treatment plan.”
Fact: FNAC can flag cancer, but a core biopsy is usually needed for the receptor tests and invasive-vs-in-situ detail before treatment is planned.
“An inconclusive result means something is badly wrong.”
Fact: It usually just means too few cells were collected. The calm next step is a core biopsy — not panic, and not a repeat of the same test.
“I need to fast or prepare specially for FNAC.”
Fact: No fasting and no injection to prepare. Wear two-piece clothing and tell your doctor about any blood-thinning medicines — that's all.
“FNAC needs stitches and days of recovery.”
Fact: There are usually no stitches. You can go home and resume normal activity the same day; a little bruising or tenderness settles within a day or two.
“A second opinion on my FNAC will offend my doctor.”
Fact: Second opinions are normal and welcomed in cancer care — they confirm the plan and give you confidence. At CION it's free when you have a report.
“A benign-looking lump doesn't need FNAC at all.”
Fact: FNAC is one of the best ways to confirm a simple cyst or fibroadenoma quickly — giving you strong reassurance instead of months of uncertainty.
Why CION
Why choose CION for your breast diagnosis
Women-headed, breast-focused
Breast and women's-health care sit at the heart of what we do — CION patients see a 1-year breast cancer survival of 96.9% vs the national 85.4%.†
Triple assessment, every time
FNAC read alongside the clinical exam and imaging — never a stand-alone verdict on a lump.
The full team, together
17 senior specialists across surgical, medical and radiation oncology plan every complex case in a tumor board.
35+ centres, 15,000+ patients
A trusted network across Telangana & AP, rated 4.8/5 by patients on Google.
Affordable & transparent
Clear costs up front, up to 50% off diagnostics, and help with insurance and EMI.
Decisions for healing, not billing
No unnecessary tests, and a free first consultation for all cancer patients.
†1-year survival. Source: ICMR / National Cancer Registry Programme (NCRP), compared with CION patient outcomes. National figures are population averages and do not predict an individual's result.
Common questions
FNAC of the breast — your questions answered
Is an FNAC of the breast painful?
For most people FNAC causes only brief, mild discomfort — similar to or less than a blood test, because the needle used is finer. You may feel a quick pinch or a little pressure as the needle goes into the lump, and the sampling lasts only a few seconds per pass. Many FNACs are done without any anaesthetic injection. Afterwards, some mild bruising or tenderness at the site is normal and settles within a day or two. If the lump is sensitive, a small amount of local anaesthetic can be used. Overall, FNAC is one of the most patient-friendly ways to check a breast lump.
What is the difference between FNAC and a biopsy?
FNAC (fine-needle aspiration cytology) uses a very thin needle to draw out loose cells, which are examined as cytology. A core needle biopsy uses a slightly thicker needle to remove a small core of intact tissue, examined as histology. The key difference is detail: a core biopsy keeps the tissue structure intact, so it can tell invasive cancer from in-situ cancer and run ER, PR and HER2 receptor tests that guide treatment. FNAC is faster and cheaper and is excellent as a first-line check, but it cannot reliably do those treatment-planning tests. Your specialist chooses based on the lump, the scan and the clinical picture.
Can FNAC detect breast cancer?
Yes — FNAC can detect cancer cells in a breast lump, and a skilled cytopathologist can identify malignant cells with high confidence. In studies of palpable breast lumps, FNAC showed roughly 74% sensitivity and 75% overall accuracy. However, no needle test alone confirms cancer with complete certainty. A clearly malignant FNAC is usually followed by a core needle biopsy before treatment, because the biopsy confirms whether the cancer is invasive and provides the receptor tests needed to plan therapy. At CION, FNAC is always read within a triple assessment alongside the clinical exam and imaging.
How accurate is FNAC of the breast?
In experienced hands with a good sample, FNAC is a reliable first-line test. A published comparative study of palpable breast lumps reported FNAC at around 74% sensitivity, 77% specificity and 75% overall accuracy, while core needle biopsy reached about 85%, 93% and 88% respectively. Combining both raised accuracy to roughly 88%. Accuracy depends on the lump's size and location, the number and quality of needle passes, and the cytopathologist's experience. This is why FNAC is interpreted as part of a triple assessment rather than alone, and why an unclear FNAC is followed by a core biopsy rather than treated as a final answer.
What happens if my FNAC result is inconclusive or inadequate?
An inconclusive or inadequate FNAC simply means the test could not give a confident answer — usually because there were too few cells or the cells were borderline. It is not a cause for alarm. The standard next step is a core needle biopsy rather than repeating the FNAC, because a core biopsy provides intact tissue and is far less likely to come back inadequate. If FNAC looked benign but your exam or scan is still worrying, a core biopsy is also done to be certain. At CION, any discordant or unclear result is moved forward through the tumor board so nothing is left hanging.
How much does FNAC of the breast cost in Hyderabad?
In Hyderabad, a standard breast FNAC typically costs between Rs. 800 and Rs. 2,400, while an ultrasound-guided FNAC usually costs around Rs. 2,000 to Rs. 3,500. The exact price depends on the centre, the cytopathologist's expertise, the number of passes taken, and whether imaging guidance is needed. A core needle biopsy, when required, is charged separately and is modestly higher. At CION we keep costs transparent and offer up to 50% off diagnostics for cancer patients, with expert-reviewed reports. Your first consultation is free — request a callback for an exact estimate.
Does FNAC need any preparation, and how long does it take?
FNAC needs very little preparation. You do not need to fast, and there is no injection to prepare for. Wear comfortable, two-piece clothing so you only need to undress from the waist up, and tell your doctor about any blood-thinning medicines or bleeding tendency, as these may need a brief check first. The sampling itself takes only a few minutes; with cleaning and slide preparation, the whole appointment is usually under 20 minutes. You can go home and resume normal activity straight away. At CION, results are explained to you by a specialist rather than simply handed over.
Why is FNAC done as part of a triple assessment?
A triple assessment means a breast lump is checked three ways — by clinical examination, by imaging (ultrasound or mammogram), and by a needle sample (FNAC or core biopsy). FNAC is done as one of those three parts because, on its own, cytology cannot tell invasive from in-situ cancer or run treatment-planning tests, and a single test can occasionally mislead. When all three parts agree, the diagnosis is highly reliable. When they disagree, it signals that more investigation is needed before any decision. At CION, this structured approach protects you from both false reassurance and unnecessary treatment, with uncertain cases reviewed by our tumor board.
Explore
Explore breast cancer care
Our complete guide to breast cancer — tests, symptoms, types, treatment, cost and recovery. Tap any topic to read more.
Worried about a breast lump? Talk to a CION specialist.
Early answers change outcomes. Book a free consultation or second opinion at any of our 9 Hyderabad clinics — part of 35+ centres across Telangana & Andhra Pradesh.
Medical disclaimer: This page is for general information and awareness and does not replace professional medical advice, diagnosis or treatment. Always consult a qualified oncologist. Costs shown are indicative only and not a quotation. Content is periodically reviewed by CION's medical team.