Breast cancer · Hormone therapy · 35+ centres across Telangana & AP
Tamoxifen for Breast Cancer: Uses, Side Effects & How Long You Take It
Tamoxifen is a daily tablet that blocks oestrogen from feeding hormone-receptor-positive breast cancer. For many women, especially before menopause, it lowers the chance of the cancer coming back. Here is what it does, the side effects you may feel, and how our oncologists help you take it for the full 5 to 10 years.
For ER/PR-positive breast cancer, including premenopausal women
Taken 5 to 10 years — decided by your tumor board
Side effects actively managed · free first consultation
★★★★★Rated 4.8/5 · 800+ Google reviews · 15,000+ patients treated
BG
Medically reviewed by Dr. Bharati Devi Gorantla, Senior Medical Oncologist — MBBS, MD, DM (Medical Oncology, Adyar Cancer Institute, Chennai), ECMO, MRCP SCE (UK), CION Cancer Clinics. · Reviewed June 2026
Start here
What tamoxifen is & who it's for
Tamoxifen is hormone (endocrine) therapy, not chemotherapy — a daily tablet that blocks oestrogen from feeding hormone-receptor-positive breast cancer cells. It belongs to a group of drugs called selective oestrogen receptor modulators (SERMs).
It is prescribed for breast cancers that are hormone-receptor-positive — meaning the tumour cells carry oestrogen receptors (ER-positive) and/or progesterone receptors (PR-positive). Roughly 7 in 10 breast cancers are hormone-receptor-positive, so tamoxifen is one of the most widely used breast cancer medicines in the world.
It is most often used after surgery (adjuvant therapy) to lower the chance the cancer returns. It is also used to treat DCIS, to treat advanced or returned hormone-positive breast cancer, and sometimes to reduce risk in women with a strong family history. Your oncologist confirms hormone-receptor status from your biopsy report before starting it. At CION Cancer Clinics, this is reviewed by our tumor board.
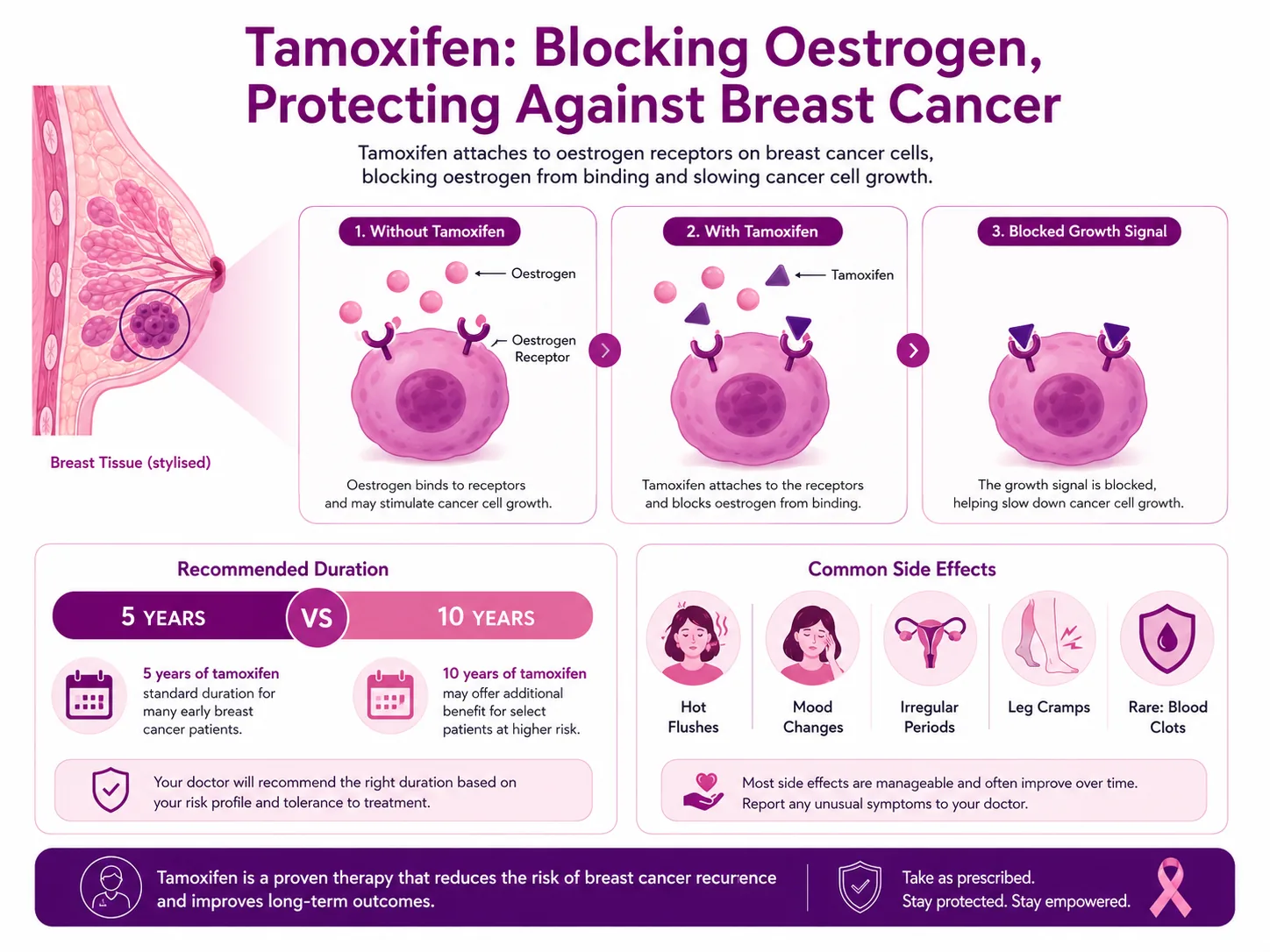
Tamoxifen sits on the oestrogen receptor and blocks oestrogen from switching the cancer cell on — cutting off the fuel that hormone-positive breast cancer needs.
The science, simply
How tamoxifen works — and how you take it
Hormone-positive breast cancer cells use oestrogen as fuel. Tamoxifen sits on the oestrogen receptor inside the cell and blocks oestrogen from attaching, so the cells stop multiplying and many die off. It is taken as a tablet — usually 20 mg once a day — so it reaches cancer cells anywhere in the body, including microscopic ones left after surgery.
Your tamoxifen journey, step by step — from confirming ER-positive disease to years of follow-up, with the team beside you at each stage.
What tamoxifen does in the body:
Blocks the receptor
Binds the oestrogen receptors on cancer cells so circulating oestrogen cannot switch them on — the core of how it works.
Slows and shrinks tumours
Starves hormone-driven cells of their fuel, reducing the chance of recurrence after surgery.
Works body-wide
A daily tablet reaches cancer cells anywhere, including the microscopic ones imaging cannot see.
Standard dose: 20 mg daily
One tablet a day, at about the same time, with or without food. Never double up a missed dose — take the next one as usual.
Did you know? About 7 in 10 breast cancers are hormone-receptor-positive, and for these tamoxifen can cut the risk of the cancer returning. Taking it for the recommended duration also reduces deaths from breast cancer — yet many women stop early because of side effects. Source: NCCN guidelines and the EBCTCG / ATLAS trial data.
Dose & duration
5 years or 10 years — how long you take tamoxifen
Five years is the proven minimum for early hormone-positive breast cancer. The ATLAS trial showed that continuing to 10 years further reduced both recurrence and deaths — with the benefit growing in the years after treatment ends. Your exact duration is a tumor-board decision, weighing your recurrence risk against side effects.
Understand each option
Simplified for understanding. Your duration and dose are decided by your oncology team for your individual case.
5 years — the proven minimum
The standard course for early hormone-positive breast cancer, and the usual duration for DCIS and risk reduction.
Up to 10 years — extended therapy
The ATLAS trial showed fewer recurrences and deaths with 10 years versus 5. Offered when your recurrence risk warrants it and you tolerate treatment well.
What to watch for
Tamoxifen side effects and how we manage them
Most women take tamoxifen for years with side effects that are manageable. The common ones are menopause-like and often ease over the first few months. The serious risks are uncommon but real — which is why regular follow-up matters. Tell your oncologist about any new symptom; many side effects can be reduced rather than endured.
Here is what to watch for and what we do about it — the common, menopause-like effects first, then the uncommon but important ones.
Hot flushes & night sweats
The most common effect, usually settling with time. Layered clothing, a cool bedroom and avoiding triggers help; if severe, we suggest non-hormonal options — never HRT.
Weight changes
Large studies did not clearly link tamoxifen itself to weight gain — it often changes from reduced activity, chemo or menopause. Our nutritionist and regular walking help.
Blood clots (DVT / PE)
A small increase in clot risk. Seek urgent care for a hot, swollen, painful calf or sudden breathlessness. Tell us before any surgery or long flight; stay mobile and hydrated.
Endometrial (womb) changes
A slightly raised endometrial cancer risk, mainly in postmenopausal women — premenopausal women are not affected the same way. Report any abnormal bleeding promptly for a gynae review.
Periods, fertility & mood
Periods may become irregular or stop, but tamoxifen is not a contraceptive. Low mood, reduced libido or dryness are common and treatable — our psycho-oncology team can help.
Eyes & rare effects
Rarely, tamoxifen can affect the eyes (including cataracts) or liver. Have an eye check if your vision changes; your liver function is monitored through routine blood tests.
Safety first
Drug & supplement interactions to avoid
Tamoxifen is switched on in the body by a liver enzyme (CYP2D6). Medicines that block it can make tamoxifen less effective, so your oncologist needs to know every tablet, supplement and herbal remedy you take. Never stop a prescribed antidepressant on your own — ask us to choose one that does not interfere.
Some antidepressants
Strong CYP2D6 blockers — fluoxetine, paroxetine, bupropion — can reduce how well tamoxifen works. Safer alternatives exist; tell us so we can adjust, not stop, your treatment.
Aromatase inhibitors
Not taken at the same time as anastrozole, letrozole or exemestane. These are sequenced, never combined with tamoxifen.
Blood thinners
Tamoxifen can increase the effect of warfarin and similar anticoagulants, raising bleeding risk. Extra monitoring is needed.
Grapefruit & alcohol
Grapefruit may interfere with how tamoxifen is processed; heavy alcohol can worsen hot flushes. Moderation is sensible.
Herbal & oestrogen products
Avoid oestrogen-containing products, and discuss any herbal supplement (including phyto-oestrogens) with us before starting it.
Is it for me?
Is tamoxifen likely to be part of your plan?
Tamoxifen is the main hormone therapy for hormone-receptor-positive breast cancer, especially before menopause. Whether it is right for you depends on your hormone-receptor status, your menopausal status and your overall plan — always decided with your oncologist and tumor board.
Quick check: might this apply to you?
Tick anything that describes your situation. This is an awareness guide, not a diagnosis or a treatment decision.
This tool doesn't decide your treatment or replace a specialist opinion. Whether tamoxifen suits you is confirmed by your oncology team from your reports.
For younger women
Fertility & pregnancy precautions
Tamoxifen must not be taken during pregnancy or breastfeeding — it can cause birth defects. Because it is not itself a contraceptive and you can still conceive, use non-hormonal contraception (such as condoms or a copper IUD) during treatment and for about two months after stopping.
If you hope to have children, raise it before you start. Fertility preservation can often be arranged, and the recent POSITIVE trial showed that some women can safely pause hormone therapy for a defined period to try for a pregnancy, then resume — a decision made carefully with your oncologist. At CION we discuss fertility openly at the first consultation, because it is far easier to plan ahead than to react later.
Do not conceive on tamoxifen
Risk of birth defects. Use reliable non-hormonal contraception during treatment and for about 2 months after stopping.
Plan fertility early
Egg or embryo preservation can often be done before starting. Tell us at the first visit if you may want children.
A planned pause may be possible
The POSITIVE trial supports a carefully timed break to attempt pregnancy for selected women — only under specialist guidance.
Worried about a side effect, or unsure whether 5 or 10 years is right for you? Book a free consultation and, if you already have a biopsy report, a free written second opinion.
Your case reviewed by a multidisciplinary tumor board
Every side effect explained and actively managed
A team decision on your dose and duration (5 vs 10 years)
9 clinics in Hyderabad · 35+ across Telangana & AP
CION cancer care is closer than you think.
We're never more than 30 minutes away. Same panel of specialists at every centre. Same tumour board reviews. Same NCCN protocols. Pick the closest one and call directly — or let us pick for you.
Don't see your city? Call
18002028726
— we'll find your nearest CION partner centre.
Meet the medical oncologists
Your hormone therapy is guided by a team, not one doctor.
Medical, surgical and radiation oncologists agree your tamoxifen plan together in a multidisciplinary tumor board — part of 17 senior specialists across CION.
Share your name and number — we'll call you back within 30 minutes to schedule your consultation.
Staying on hormone therapy is easier with a team beside you.
Free first consultation for all cancer patients — confidential, doctor-led, and never rushed. We help you take tamoxifen for the full course, with side effects managed.
Worry and misinformation keep people from the least invasive option. Here are the beliefs we hear most, and the facts.
“Tamoxifen is chemotherapy.”
Fact: It is hormone therapy, not chemo — a daily tablet that blocks oestrogen. It does not cause the hair loss or low blood counts typical of chemotherapy.
“Tamoxifen will make me gain a lot of weight.”
Fact: Good research does not clearly link tamoxifen itself to weight gain. Weight often changes from reduced activity, chemotherapy or menopause rather than the tablet.
“Tamoxifen will give me uterine cancer.”
Fact: The risk is small and mainly affects postmenopausal women; premenopausal women are not affected the same way, and the benefit far outweighs it. Report any abnormal bleeding promptly.
“Once I feel well I can stop taking it early.”
Fact: Stopping early raises the chance the cancer returns. The protection comes from finishing the full course — most side effects can be managed so you can stay on it.
“5 years is always enough — 10 years is pointless.”
Fact: For the right patients the ATLAS trial showed that continuing to 10 years further reduced both recurrence and deaths from breast cancer.
“Tamoxifen works as contraception, so I can't get pregnant on it.”
Fact: It is NOT a contraceptive and can cause birth defects. Use reliable non-hormonal contraception during treatment and for about two months after stopping.
“I can't take tamoxifen because I'm premenopausal.”
Fact: Tamoxifen is the main hormone therapy before menopause — aromatase inhibitors do not work on their own in premenopausal women.
“Side effects mean the drug is harming me, so I should stop.”
Fact: Most side effects are manageable and often ease over the first few months. Tell your oncologist — many can be reduced rather than endured.
“I can keep taking my usual antidepressant and supplements without mentioning them.”
Fact: Some (like fluoxetine and paroxetine) can make tamoxifen less effective. Tell us so we can switch you safely — never stop a prescribed medicine on your own.
“A second opinion on my hormone therapy will offend my doctor.”
Fact: Second opinions are normal and welcomed in cancer care — they confirm the plan and give you confidence. At CION it's free when you have a biopsy report.
Why CION
Why choose CION for your hormone therapy
A dedicated cancer network
CION treats cancer and only cancer — focused, patient-specific care, not a general hospital's approach.
Tumor board for every case
Medical, surgical and radiation oncologists agree your tamoxifen plan and duration together — never one opinion.
Close to home
9 clinics across Hyderabad and 35+ centres across Telangana & AP, so years of follow-up don't mean long journeys.
Structured side-effect reviews
Regular check-ins catch and treat hot flushes, mood changes and other effects early, so you can keep taking the tablet.
Bleeding & gynae monitoring
Prompt gynaecology review for any abnormal vaginal bleeding, with clear advice on what to watch for at home.
Support through the years
Nutrition and psycho-oncology help you manage weight, energy and mood across the full 5 to 10 years.
Common questions
Tamoxifen — your questions answered
Is tamoxifen chemotherapy?
No. Tamoxifen is hormone (endocrine) therapy, not chemotherapy. It works by blocking oestrogen from feeding hormone-receptor-positive breast cancer cells, rather than by destroying fast-dividing cells the way chemotherapy does. That is why it is taken as a daily tablet at home and does not cause the hair loss or low blood counts typical of chemo. Some women have chemotherapy first and then take tamoxifen afterwards to lower the chance of the cancer returning. Your oncologist will explain exactly where tamoxifen fits in your overall treatment plan.
Should I take tamoxifen for 5 years or 10 years?
It depends on your individual risk of recurrence. Five years is the proven minimum for early hormone-positive breast cancer. The ATLAS trial showed that continuing to 10 years further reduced both recurrence and deaths from breast cancer, with the benefit growing in the years after treatment. For premenopausal women, guidelines support starting with 5 years and continuing to 10 if you remain premenopausal and are tolerating it well. At CION this decision is reviewed by our tumor board, weighing your recurrence risk against side effects, so you get a team recommendation rather than a one-size answer.
Does tamoxifen cause weight gain?
Although weight gain is sometimes listed as a side effect, good research does not show a strong link between tamoxifen itself and gaining weight. One study of over 3,000 breast cancer survivors found tamoxifen was not clearly associated with weight gain, while chemotherapy was. Weight often changes during treatment because of reduced activity, menopause or other medicines rather than the tamoxifen tablet. Regular walking, a balanced diet rich in vegetables and lean protein, and support from our nutritionist all help. If you are gaining weight and it worries you, tell your oncologist so other causes can be checked.
Can tamoxifen cause uterine or endometrial cancer?
Tamoxifen can thicken the lining of the womb and slightly increases the risk of endometrial cancer, but this risk mainly applies to postmenopausal women; premenopausal women are not affected in the same way. The overall risk is small and is far outweighed by tamoxifen's benefit in preventing breast cancer recurrence. The key safety step is simple: report any abnormal vaginal bleeding to your doctor promptly so it can be investigated early. At CION we arrange a gynaecology review for any unexpected bleeding, because problems found early are the most treatable.
What should I avoid while taking tamoxifen?
Tell your oncologist about every medicine and supplement you take, because some interact with tamoxifen. Certain antidepressants (fluoxetine, paroxetine, bupropion) can make it less effective, so these should be reviewed rather than stopped on your own. Avoid taking tamoxifen at the same time as aromatase inhibitors. Grapefruit and grapefruit juice may interfere with how the drug is processed, and heavy alcohol can worsen hot flushes. Avoid oestrogen-containing products and discuss any herbal remedy before using it. Do not get pregnant while taking tamoxifen, as it can cause birth defects.
Is it safe to get pregnant on tamoxifen?
No. Tamoxifen can cause birth defects, so you must not be pregnant or breastfeed while taking it. Because it does not act as a contraceptive and you can still conceive, use non-hormonal contraception (such as condoms or a copper IUD) during treatment and for about two months after stopping. If you hope to have children, raise it before you start so fertility preservation can be arranged. The recent POSITIVE trial showed that some women can safely pause hormone therapy for a planned time to try for a pregnancy and then resume — a decision made carefully with your oncologist.
When do tamoxifen side effects start, and do they go away?
Common side effects such as hot flushes, night sweats or mild nausea often begin within the first few weeks and frequently ease over the first few months as your body adjusts. Some effects, like changes to periods, may persist while you are on treatment. Serious effects such as blood clots or abnormal womb bleeding are uncommon but need prompt attention at any point. The most important thing is not to suffer in silence: most side effects can be reduced through simple measures, dose timing or supportive care. Tell your CION oncologist about anything new at your follow-up visits.
Can I take tamoxifen if I am premenopausal?
Yes — tamoxifen is the main hormone therapy for premenopausal women with hormone-receptor-positive breast cancer. This is because aromatase inhibitors do not work on their own before menopause. Depending on your risk, your oncologist may combine tamoxifen with ovarian suppression for added protection. Premenopausal women also do not carry the same endometrial cancer risk that postmenopausal women do. Because younger women face issues around periods, fertility and pregnancy, we discuss all of this openly at your first 45-minute consultation so your plan fits your life as well as your cancer.
Explore
Explore breast cancer care
Our complete guide to breast cancer — surgery, diagnosis, treatment, types, symptoms and recovery. Tap any topic to read more.
On tamoxifen, or about to start? Talk to a CION oncologist.
Staying the course is easier with a team beside you. Book a free consultation or second opinion at any of our 9 Hyderabad clinics — part of 35+ centres across Telangana & Andhra Pradesh.
Medical disclaimer: This page is for general information and awareness and does not replace professional medical advice, diagnosis or treatment. Always consult a qualified oncologist. Costs shown are indicative only and not a quotation. Content is periodically reviewed by CION's medical team.