A patch of breast skin that looks pitted, thickened and swollen, with tiny dents where the hair follicles are tugged inward. Run a finger over it and the surface feels bumpy and tight rather than smooth.
Peau d'orange is not a disease on its own. It is a visible sign that fluid is building up under the skin of the breast. The important question is always the same: what is causing that fluid to collect? The answer ranges from a harmless infection to inflammatory breast cancer, which is why a new orange-peel change should never be ignored or watched for weeks at home.
It also helps to know the words doctors use for related changes:
A single pulled-in dent.
Skin drawn inward like a seam.
A wider area of pitting and swelling.
Any of these, when new, deserves a clinical look.
A patch of skin that is pitted and dimpled like an orange peel, often slightly raised, swollen or shiny.
Thicker and tighter than the surrounding breast skin; sometimes warm or tender.
It is not a diagnosis by itself. It is a sign that something underneath needs to be explained.
Inflammatory breast cancer is rare — only about 1 in 40 breast cancers — but it is one of the most aggressive forms, and orange-peel skin (peau d'orange) is one of its hallmark signs. Because it often produces no distinct lump and can look exactly like a breast infection, it is frequently mistaken for mastitis at first and diagnosed late. That is why any new, rapidly spreading orange-peel or red patch on the breast should be reviewed by a specialist within days, not weeks. (Source: American Cancer Society / NCCN guidelines on inflammatory breast cancer)
Breast examination, mammography and ultrasound coordination, MRI, and same-day expert-reviewed PET-CT happen at the centre nearest you. Every complex breast case is reviewed by the same tumor board, so wherever you walk in, you get a team's opinion — not one doctor's guess.
Not sure which centre fits best? Tell us where you are — we'll suggest the closest one with the right specialists.
Help me pick the right centreTravelling for treatment? We may have a centre right where you are.
Don't see your city? Call 18002028726 — we'll find your nearest CION partner centre.
Trained at AIIMS, Tata Memorial and leading international centres, with 150+ years of combined experience. Every complex breast case is reviewed by our tumor board — several specialists together, not one opinion.


MBBS(Gold Medal), DNB(General Medicine), DM(Medical Oncology)(Gold Medal)

MBBS, MD(General Medicine), DM(Medical Oncology)(Adyar,Chennai), ECMO, MRCP SCE(UK)

MBBS, MD (General Medicine), DrNB (Medical Oncology), ECMO, MRCP SCE (Medical Oncology) (UK)



MBBS (AIIMS), MS (Surgery) (AIIMS), DNB (Surgical Oncology), MRCS (Edinburgh)



MBBS, MS(General Surgery), M.Ch(Surgical Oncology), FMAS, FARIS(Ongoing)






MBBS, MS (General Surgery), DrNB (Surgical Oncology), FALS Oncology

Want a specific doctor for your case? Mention them when booking.
Book Free ConsultationShare your name and number — we'll call you back within 30 minutes to schedule your consultation.
Lymphatic vessels in the breast skin become blocked or overwhelmed and stop clearing fluid.
Lymph collects in the skin (oedema), making the breast feel swollen, heavy or tight.
Hair follicles stay anchored while the skin around them swells, creating the pitted orange-peel pattern.
Several conditions can produce peau d'orange. Some are harmless and settle with simple treatment; one is a medical emergency. Because the skin looks similar in all of them, the safest approach is to have any new orange-peel change examined rather than guess. Below are the causes doctors weigh up.
The cause that makes peau d'orange urgent. IBC is rare — roughly 1 in 40 breast cancers — but it is fast-growing. Instead of a single lump, cancer cells block the lymphatic vessels in the breast skin, causing rapid redness over a third or more of the breast, warmth, swelling and orange-peel skin, often appearing over days to weeks. Because it can look exactly like a breast infection, it is sometimes missed at first. Any orange-peel change that does not clearly settle within a week needs specialist review and usually a biopsy.
An infection of the breast tissue, most common during breastfeeding, can cause redness, pain, warmth, fever and swollen, orange-peel skin. Mastitis usually improves within a few days of antibiotics. The critical safety rule is this: if a 'breast infection' does not clearly clear up with a short course of antibiotics, it must be re-examined for inflammatory breast cancer, because the two look almost identical at the start.
Swelling caused by impaired lymphatic drainage — for example after breast surgery, lymph-node removal or radiation, or from other blockage — can leave the breast or arm skin thickened and pitted. Lymphedema is managed with specialist lymphatic therapy, compression and skin care once cancer has been ruled out as the cause.
Trauma, a knock, a previous biopsy or surgery can leave an area of dead fat tissue (fat necrosis) that tethers the skin and mimics dimpling or orange-peel skin. Benign fibrocystic changes can do the same. These are not cancer and do not raise future cancer risk, but they should still be confirmed by examination and, if needed, imaging so nothing more serious is overlooked.
Less commonly, generalised fluid retention from heart, kidney or thyroid conditions, certain connective-tissue diseases, an allergic reaction, or recent radiotherapy to the breast can produce orange-peel skin. These are diagnosed alongside a full clinical picture rather than from the skin alone.
Talk to a CION breast specialist today and get a clear next step, free of charge.
Evaluating peau d'orange is about answering one question safely and quickly: is this a benign cause, or is it inflammatory breast cancer? A specialist works through the steps below. The aim is no unnecessary tests, but also no missed diagnosis — every step has a clear reason.
Your specialist examines both breasts and the armpit and underarm lymph nodes, and asks how fast the change appeared. Speed of onset is a key clue: inflammatory breast cancer typically develops over days to a few weeks. A full 45-minute consultation gives time to take this history properly rather than rushing it.
Ultrasound and mammography look beneath the skin for thickening, masses or abnormal lymph nodes and guide the next steps. An important caveat your doctor will explain: inflammatory breast cancer does not always form a visible lump, so a 'clear' mammogram alone is not enough to rule it out.
Because mammograms can miss inflammatory breast cancer, an MRI of the breast is often added. MRI is more sensitive to the diffuse skin and tissue changes of IBC and helps map how much of the breast is involved before any treatment decision.
The step that gives a definite answer is a biopsy. A core biopsy samples any abnormal tissue, and a skin punch biopsy samples the affected skin to look for cancer cells blocking the dermal lymphatics — the finding that confirms inflammatory breast cancer. A biopsy is the only way to be certain whether peau d'orange is cancer or not.
If a biopsy confirms cancer, staging investigations such as a PET-CT and blood tests check whether it has spread, so the team can plan the right combination of treatment. CION offers expert-reviewed PET-CT with same-day reporting.
If a breast infection is the likely cause, a short course of antibiotics may be tried first. The safety rule every CION clinician follows: if the skin does not clearly improve within about a week, the case is escalated for biopsy rather than treated as infection again — this is how early inflammatory breast cancer is caught.
At CION, 1-year survival for breast cancer in our patients is 96.9%, against a national average of 85.4% — a difference of +11.5 percentage points.* No clinic can promise a cure for any one person, and we never will. But getting a confident, tumor-board-backed diagnosis quickly is the single most useful thing you can do when you notice orange-peel skin.
*1-year survival. Source: ICMR / National Cancer Registry Programme (NCRP). Individual outcomes vary by stage, biology and overall health.
No. Orange-peel skin (peau d'orange) is a sign that fluid is building up under the breast skin, and it has several possible causes. Many are harmless, such as a breast infection (mastitis), lymphedema, fat necrosis after an injury, or benign breast changes. However, it can also be the first sign of inflammatory breast cancer, which is rare but fast-growing. Because the skin looks similar in all of these, the appearance alone cannot tell you the cause. The safe approach is to have any new orange-peel change examined promptly rather than assume it is harmless or assume the worst.
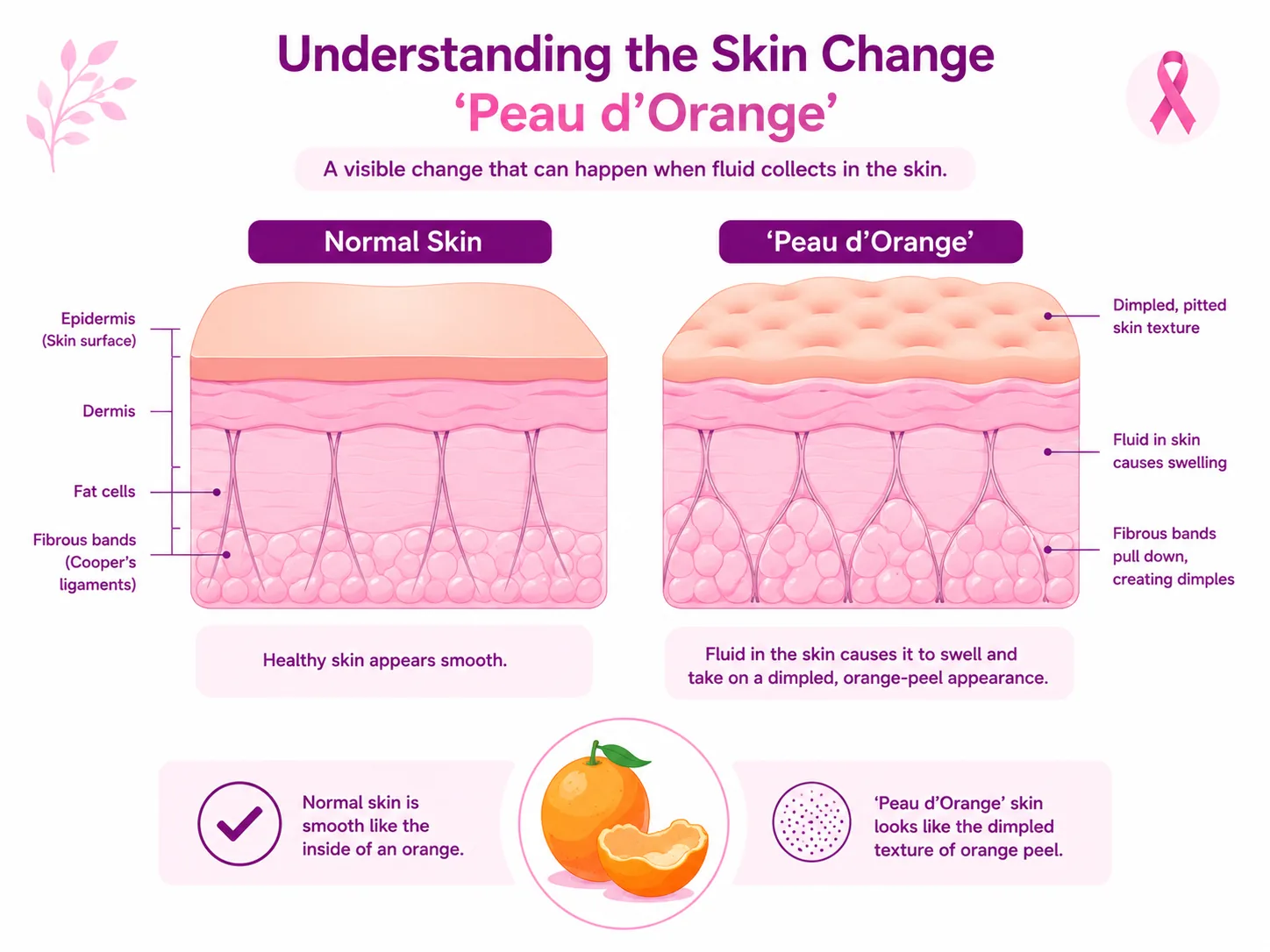
Peau d'orange skin feels thicker, tighter and bumpier than the normal smooth skin around it. The surface is pitted with small dents, like the skin of an orange, and the area is often swollen and may feel warm or tender. Some people notice the breast looks shiny, slightly larger or heavier than the other side. It is different from a single dimple (a localised pulled-in dent) because it usually covers a wider patch. If you can feel or see this kind of change and it is new, have it checked.
The orange-peel look comes from blocked lymphatic drainage in the breast skin. Tiny lymph channels that normally carry fluid away become blocked or overloaded, so fluid collects and the skin swells. Meanwhile, hair follicles stay anchored to the deeper tissue, so as the skin around them puffs up, those points get pulled inward. The combination of swelling plus tethered follicles produces the pitted, dimpled, orange-peel pattern. In inflammatory breast cancer, the same blockage happens because cancer cells plug the skin's lymphatic vessels.
Do not wait. Book a review as soon as you notice a new orange-peel, dimpled or rapidly reddening area on a breast. Inflammatory breast cancer can develop over just days to weeks, so 'watching it' at home can allow a serious cause to advance. Even if a breast infection seems likely and you are given antibiotics, the key safety rule is that the skin should clearly improve within about a week — if it does not, you need to be re-examined and usually have a biopsy. When in doubt, get it looked at early; most causes are treatable, and the serious one is the one you most want to catch quickly.
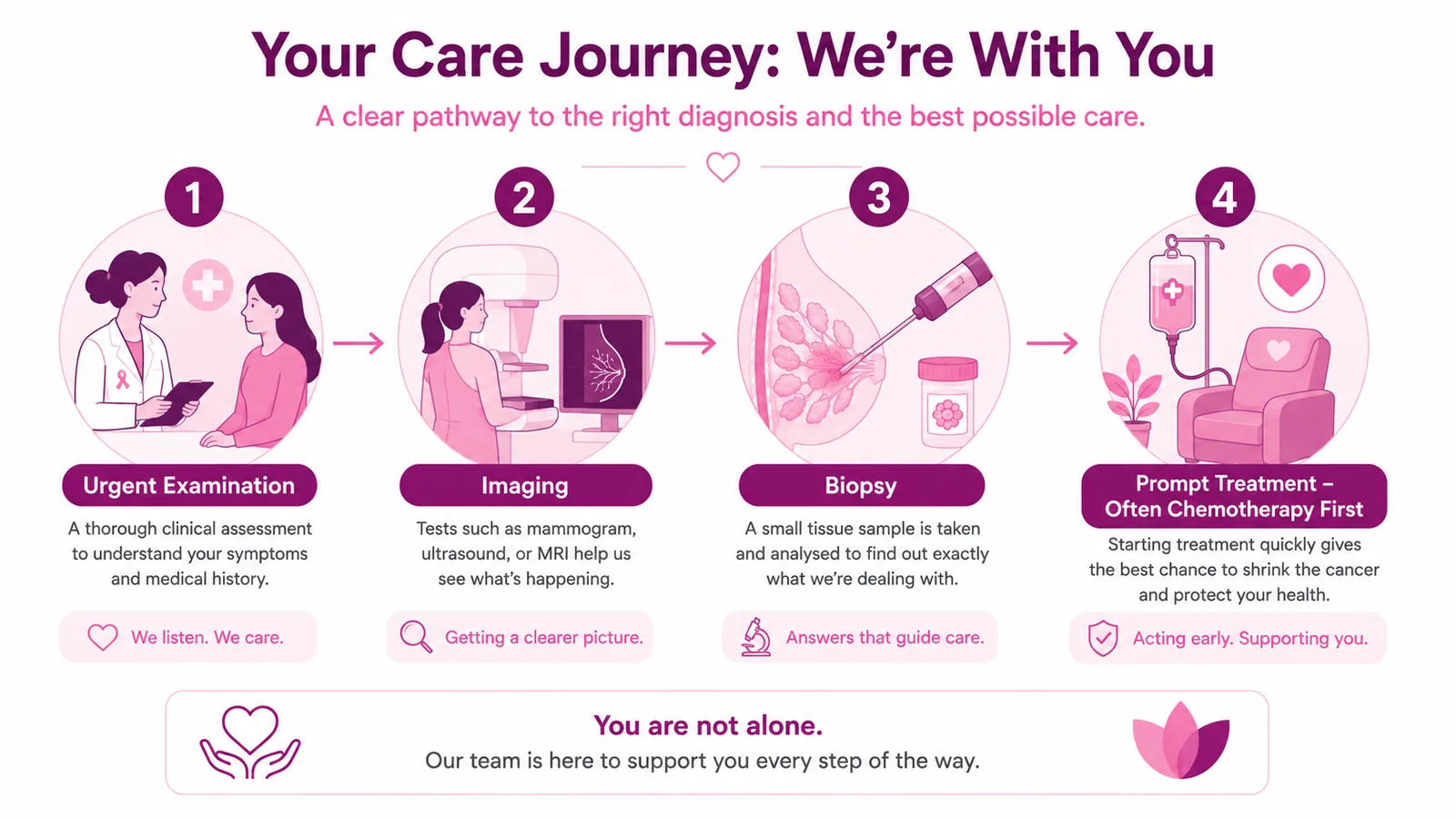
Diagnosis starts with a detailed clinical examination of both breasts and the underarm lymph nodes, including how quickly the change appeared. Your specialist will usually arrange breast imaging — ultrasound and a mammogram — and often an MRI, because inflammatory breast cancer does not always form a visible lump and can be missed on a mammogram alone. The step that gives a definite answer is a biopsy: a core biopsy of any abnormal tissue and a skin punch biopsy of the affected skin to look for cancer cells blocking the lymphatic vessels. If cancer is confirmed, staging scans such as PET-CT check whether it has spread.
They are related but not the same. Dimpling is usually a single dent where the skin is pulled inward at one point, sometimes only visible when you raise your arms. Puckering is skin drawn in like a seam. Peau d'orange is a broader patch of pitted, swollen skin that resembles an orange peel, caused by widespread fluid build-up in the skin. All three are skin changes worth checking when they are new, but peau d'orange in particular, especially with redness and rapid swelling, raises concern for inflammatory breast cancer and should be evaluated quickly.
Yes. Once cancer has been ruled out, the treatment depends on the cause. A breast infection (mastitis) is usually treated with antibiotics and often resolves within days. Lymphedema is managed with specialist lymphatic therapy, gentle compression and careful skin care. Fat necrosis and benign breast changes often need no treatment beyond confirmation and reassurance. Skin swelling from general fluid retention is treated by addressing the underlying condition. The first priority, though, is always a confident diagnosis — so the right treatment is matched to the right cause and nothing serious is missed.
CION Cancer Clinics is a woman-headed, tumor-board-led group with 17 super-specialist oncologists, more than 150 years of combined experience, and 35+ centres across Telangana and AP. Every complex breast case is reviewed by medical, surgical and radiation oncologists together, so you get a team's opinion rather than one doctor's view. We offer a free first consultation, a full 45-minute appointment so nothing is rushed, fast diagnostics including same-day expert-reviewed PET-CT, and transparent costs with no unnecessary tests. CION's 1-year breast cancer survival is 96.9% versus a national average of 85.4% (ICMR/NCRP). Outcomes vary by individual, and we never promise a cure — but we do promise a clear, fast, honest path forward.
Medical Disclaimer: The information on this page is provided for general educational purposes and reflects current clinical practice in breast oncology at the time of last medical review. It is not a substitute for individual medical advice, diagnosis, or treatment. Orange-peel breast skin can have many causes, and only a qualified physician examining you can determine which applies. Survival statistics cited are population-level estimates and do not predict outcomes for an individual case.
Browse our complete guide to breast cancer — types, symptoms, tests and treatments. Tap any topic to read more.